Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
17-SEPTEMBER-2016 AMAL SHAABAN
AL-JABALY 53 YEARS INTRADURAL EXTRAMEDULLARY MENINGIOMA C1-3 RIGHT SIDE.
Anamnesis
The patient came to the clinic
03-September-2016 complaining of neck and right
upper limb pain for 4 years with
progressing numbness right hand. MRI cervical
spine spine performed 01-September-2016 without
report and very bad quality, showing as be an
intramedullary mass behind C1-2-3.
On examination, the patient had no pain when
turning the head to all direction. There is weak
right deltoid 3/5, left 4/5, right biceps -4/5,
left 4/5, flexion right hand 3/5, left 4/5,
extension right hand -3/5, left 3/5, right
triceps 4/5, left 5/5. There is weak
dorsiflexion right foot -4/5, left 4/5. The deep
reflexes were exaggerated in the right side, but
no pathologic reflexes. There is no apparent
sensory deficit.
The patient was sent for thorough investigations
and MRI cervical spine performed
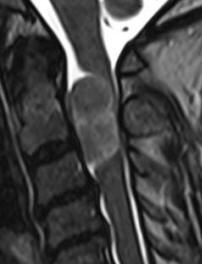
04-September-2016 showing huge meningioma
33x12.7 mm intradural pushing the spinal cord to
the left. Spectroscopy was typical for
meningioma and the mass was lacking fibers.
There is and extension to the right C1-2 foramen
reaching the vertebral artery pushing it
anterior.
In prone position with the
use of IOM ISIS, laminectomy of C2-3 and partial
of C1 was
achieved. The dura was opened slightly right
parallel to the midline. The dumbbell-shaped
appearance of the tumor was due to right C2
anterior and posterior rootlets, which were
constricting the tumor and they were preserved
to the end of surgery. The matrix of the
meningioma was the right lateral wall of the
dura, which was coagulated and piece-meal
resection of the tumor was performed. MEP was
troubleshooting and not informative. After the
resection of the tumor a tiny piece and the
emergence of the right C1 was removed trying
during that to preserve the rootlets. Using MultiGen, bipolar motor stimulation of
right C2 was achieved with 1.0 V. Motor stimulation
of the right side of the spinal cord and a brisk
response of the right upper and lower limbs was
achieved above the tumor resection area.
Irrigation of the area with 1 ampoule Papaverine
diluted with 20 ml saline. The dura was closed
water-tightly. Routine closure of the
wound. The patient was sent to MRI before
extubation.
Smooth postoperative recovery. She
showed deep paralysis of the right upper and
lower limbs, which started to improve over
several hours. She was sent to the ICU.
MultiGen
Follow
Up
The patient came 03-October-2016 to the clinic
walking without aid: The motor function
normalized and having numbness left side of the
body. The postoperative recovery was amazingly
excellent. The wound was clean and she suffered
from occipital headache with neck pain.
Comments
The patient has huge meningioma
compressing the spinal cord. The clinical course is
progressive and surgical removal is the only option.
This is the 81st case using the MultiGen. This procedure regained routine acceptance.
It
became
a usual part of the spine surgery.
Click here for
reference.
With presence of motor response of the
spinal cord above the resected tumor with threshold of 1 V,
it tells that in worst scenario, the the paraplegia will be
transient.
Nor MRI or CT-scan can give precise real
picture of the morphological event. This case is a
demonstration, of how DTI still not showing the full
picture, and spectroscopy needs more perfection.
Intraoperative neurophysiologic
monitoring is a must in this case to avoid catastrophic
events.
Intraoperative MRI after resection of
tumor can assure the total resection of the tumor and the
condition of the spinal cord after removal.
Irrigation with Papaverine is a must to
prevent arterial spasm.
In this case ILLICO mini retractor system
was of great help.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
ILLICO minimally retractor system
The meningioma in different sections and sequences.
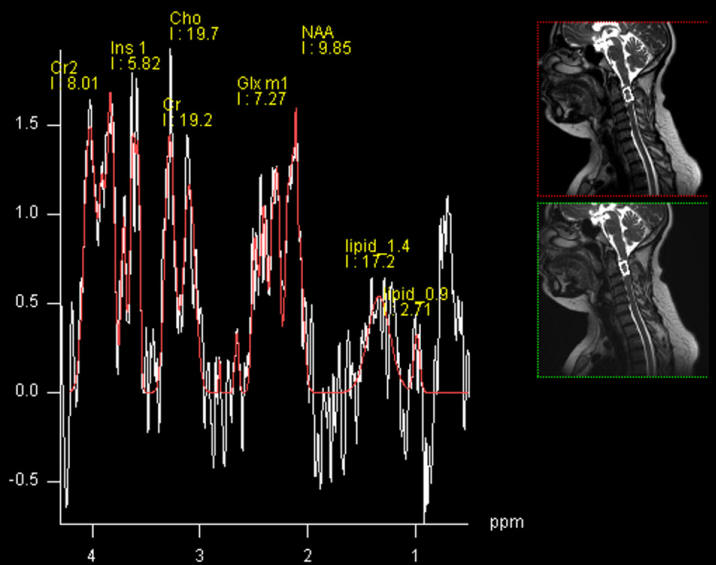
Single voxel Spectroscopy showing the peak at 3.8 ppm characteristic
for meningiomas. For more information,
click
here!
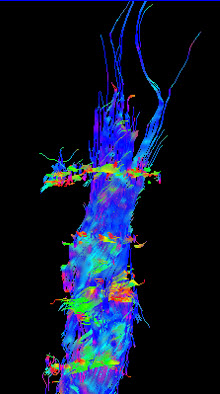
DTI showing absence of fibers confirming nonglial nature of the
mass.
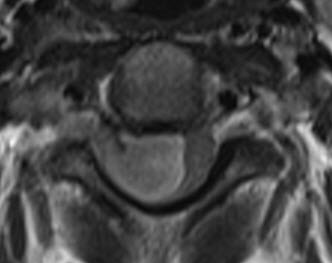
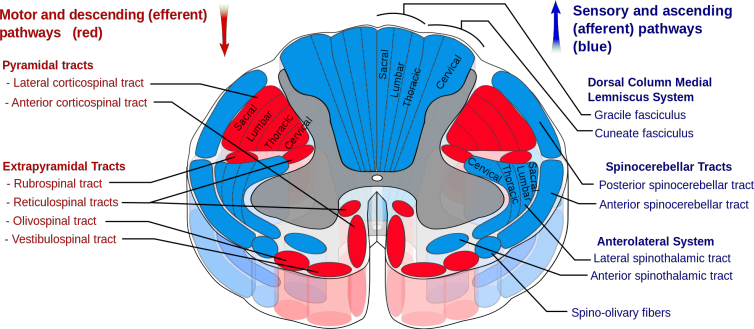
Anatomical architecture of the spinal cord at C2-C3 level.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .