| Case Presentation: | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
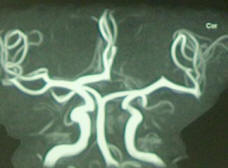
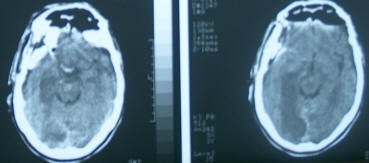
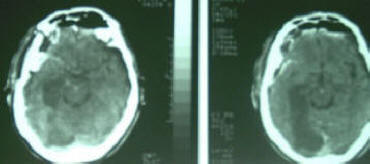
A Syrian gentleman 58 years came to the clinic 05-11-2004 with complaining of right oculomotor plegia. He was referred as a case of meningioma and he was sent for more MRI and MRA investigations, which confirmed the diagnosis of right posterior clinoid meningioma. The patient start to complain of Diplopea for 2 days then the last 2 weeks progressed complete right oculomotor plegia. The patient was admitted to Al-Shmaisani hospital 09-11-2004 and was operated the same day: Wide right fronto-temporal approach with tranzygomatic route was achieved and the tumor was morphologically identical for meningioma with matrix and carpet of meningial involvement. It was engulfing the supraclinoid ICA and pushing the M1 and the solitary A1 upward. The tumor was radically removed with preservation of all even tiny anatomical structures, including the anterior choroidal artery, the right PcoA, the right ICA, right optic nerve and the compressed right oculomotor nerve. The Liliquist membrane was opened for 2 mm distance to ensure that the oculomotor nerve was in continuity. No attempt was intentionally direct to explore the basilar and PCAs, to avoid manipulations and slipping of blood to that region. The operation was straight forward without any unusual events and the preliminary frozen section was suspecting the non-meningioma histologic verification, which could not be believed at that time. Even with this consideration total resection of the lesion was achieved. The patient awakened from G.A. He was sent to ICU and he was drowsy. The breathing pattern was acceptable, but he was aphasic with left side hemiparesis. Considering the smooth operation, CT-scan done immediately after operation and the CT-findings were acceptable. The next day, the condition was the same, for what another CT-scan done and showed massive infarction in the territory of both PCAa more pronounced in the right side. The patient despite vigorous efforts to treat the seemingly infarcted area, progressed to deteriorate. Immunohistologic results were of highly malignant endocrine carcinoma. Considering that the patient was transferred from Syria , after putting him in ventilator in tracheostomy was performed 18-11-2004 to wean him off ventilator the next day. He was transferred to Syria 20-11-2004, and after some improvement, he was discharged to home to die 01-12-2004. Comments: Endocrine carcinoma is one of the most malignant tumors. It took here an aggressive course and the patient died within one month from the start of his illness. The strange point here to mention, that this tumor was unbelievable 100% grossly resembling a meningioma. The cascading catastrophic events also remain unexplained, since vasospasm was taken into account and precautionary measures were undertaken to prevent such event. The lesion was not related to the hypothalamus nor to the hypophysis. This interesting case is lacking more detailed investigations due to economic and geographic factors.
Related topics: |
|
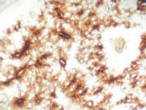
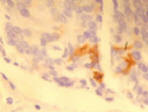 The immuno-histologic study of the endocrine carcinoma with syntaptophysin stain
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()