Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
19-AUGUST-2008 AHMAD FAYSAL OEDEH 38 YEARS
MALIGNANT HIGH GRADE ASTROCYTOMA LEFT TEMPORO-FRONTAL LOBES WITH IMPENDING
CONNING.
Anamnesis:
The patient came to the
clinic 12-August-2008 complaining of left sided
headache for 20 days with repetitive
sensory-motor Jacksonian attacks in the right
side of the body taking place several times
daily. The patient came from a hospital were
they were treating him for encephalitis.
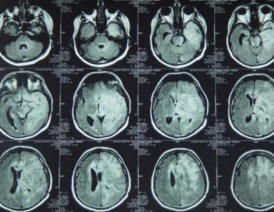
CT-scan of the brain done
11-August-2008 showed left fronto-temporal mass.
MRI done 12-August-2008 confirming the presence
of wide-spread mass infiltrating the left
fronto-temporal lobes with shifting of the
midline structures and pending conning.
High-grade astrocytoma was in the top of the
diagnosis and glioblastoma multiforme could be
the second in the list.
On examination: Romberg was
stable with no signs of cerebellar dysfunction,
except for fine tremor of the right hand. There
was no meningism and he had mild paresis of the
right limbs more in the distal muscles with
flattened right naso-labial fold. The patient is
left handed, but using the right hand.
The patient was advised to
repeat MRI of the brain with contrast with MRA
and MRV of the brain to be performed after 3
days. It was done and the mass still the same.
It was advised that
performing surgery without using gliadel wafers.
could yield relatively bad prognosis. The
relatives agreed and 16 wafers were ordered.
Left temporal approach was
performed and the bone flap was reflected to the
left ear. Despite the use of aggressive
dehydration and hyperventilation and all
measures to decrease the intracranial pressure,
the dura was stony tense. It was decided to make
a mini-incision over the lower temporal gyrus.
Suction of the tumor was performed from this
incision with the use of bipolar, because the
tumor was rich in vascularity with abnormal
vessels running inside it. Frozen sections
revealed the presence of high grade astrocytoma.
After the dura became
relatively lax, the dura was opened more wide
and not reaching the sylvian cistern and not
reaching the junction of the vein of Labbe.
The resection was limited 10
mm away from the sylvian cistern, so as to avoid
any mechanical irritation of the left MCA
branches and 10 mm away from the edge of the
tentorium in the plan so as to avoid any contact
with the brainstem. The upper temporal gyrus was
preserved so as not to cause any damage to the
Broca and Wernike-Mann areas. Taking these areas
into consideration and the use of Inomed IOM
intraoperative navigation, it was possible to
remove a plenty part of the tumor with a cavity
inside the temporal lobe. After achieving
heamostasis, the 16 Gliadel wafers were
implanted in the cavity of the tumor bed and
over the tumorous cortex of upper temporal
gyrus. Tachyseal was covered over the the wafers
and the dura was stitched . Over the dura
another layer of Tachyseal was used.
Routine closure of the wound
and smooth postoperative recovery with smooth
postoperative recovery.
Comments
The patient has very
aggressive tumor. Surgery alone is not a
sufficient option. Using Gliadel wafers could
improve the long-term outcome.
Usually radiotherapy will be
planned after 4-5 weeks after surgery.
In case that the dura is very
tense before opening, if the conservative
measures fail to decrease the pressure, it is
advisable to perform small dural incision and
perform decompression, after what the dura can
be widened to prevent brain from bulging and
secondary brain damage due to shift and vein
cutting at the edge of the dura.
Please! wait for 3-5 min till the
video start to load. It depends upon the internet
connection.
Follow Up
09-June-2010: The patient was
put under observation and underwent radiation
therapy over 6 weeks 2 months after
surgery. He showed improvement and the patient
temozolomide for several months. The last 3
months, the control MRI start to show
morphological deterioration, but clinically he
was stable. The last week he became with
obtundation with gross right hemiplegia with MRI
confirming escalation of the tumor borders. The
patient was put in massive doses of Decadron
after what he slightly improved. Avastin
5 mg/Kg with CAMPTO 700 mg were given
07-June-2010. The patient tolerated the first
course without complications. The duration
of his disease up to now is almost 2 years.
During the course of temozolomide, it was
clear that there was morphological regression of the tumor
with improvement of his neurological status, but after one
year of therapy, the medication became ineffective.
The combination of the Avastin and CAMPTO
was applied by the recommendations of J. J. Vredenburgh
et.al (Journal of Clinical Oncology Volume 25 Number 30
October 20 2007).
After 2 courses of Avastin
and CAMPTO the patient showed considerable
clinical improvement with improvement of the
right sided paresis and the patient became fully
alert with ability of ambulation with help.
MRI 03-June-2010 before
Avastin and CAMPTO
MRI 01-July-2010 after 2
courses
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .