|
Becker's muscular dystrophy (also known as
Benign pseudohypertrophic muscular dystrophy) is an
X-linked recessive inherited disorder
characterized by slowly progressive muscle weakness
of the legs and
pelvis.
It is a type of dystrophinopathy, which includes a
spectrum of muscle diseases in which there is
insufficient dystrophin produced in the muscle
cells, resulting in instability in the structure of
muscle cell membrane. This is caused by
mutations in the dystrophin
gene,
which encodes the
protein
dystrophin. Becker's muscular dystrophy is
related to
Duchenne muscular dystrophy in that both result
from a mutation in the dystrophin gene, but
in Duchenne muscular dystrophy no functional
dystrophin is produced making DMD much more severe
than BMD. Both Duchenne and Becker's muscular
dystrophy have traditionally been called "X-linked"
recessive diseases, but in view of modern molecular
biology and identification of the dystrophin gene,
it might be more appropriate to say they are
X-chromosome recessive diseases. Becker's is named
after the German doctor
Peter Emil Becker.
 Genetics
Genetics
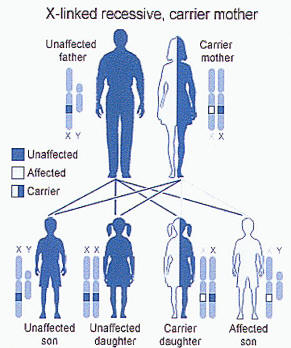
The disorder is inherited with an
X-linked recessive inheritance pattern. The gene
is located on the X
chromosome. Since women have two X chromosomes,
if one X chromosome has the non-working gene, the
second X chromosome will have a working copy of the
gene to compensate. In these cases, some women have
much milder symptoms because of this ability to
compensate. For example, carrier females of
mutations are at increased risk for
dilated cardiomyopathy. Since men have an X
and a Y chromosome and because they don't have
another X to compensate for the defective gene, they
will develop
symptoms if they inherit the non-working gene.
All dystrophinopathes are inherited in an
X-linked recessive manner. The risk to the siblings
of an affected individual depends upon the carrier
status of the mother. Carrier females have a 50%
chance of passing the DMD mutation in each
pregnancy. Sons who inherit the mutation will be
affected; daughters who inherit the mutation will be
carriers. Men who have Becker's muscular dystrophy
can have children, and all their daughters are
carriers, but none of the sons will inherit their
father's mutation.
Prenatal testing through
amniocentesis or
chorionic villus sampling (CVS) for pregnancies
at risk is possible if the DMD mutation is found in
a family member or if informative linked markers
have been identified.
Becker's muscular dystrophy occurs in
approximately 3 to 6 in 100,000 male births.
Symptoms usually appear in men at about age 12, but
may sometimes begin later. The average age of
becoming unable to walk is 25-30. Women rarely
develop symptoms.
Genetic counseling is indicated for individuals
or families who may carry this condition. Also
enlarges reproductive organs.
Symptoms
- Muscle weakness, slowly progressive
(Difficulty running, hopping, jumping;
Progressive difficulty walking)
- Ability to walk may continue into
adulthood (up to age 40)
- Frequent falls
- Difficulty
breathing
- Cognitive dysfunction
-
Skeletal deformities,
chest and
back
(scoliosis)
- Muscle deformities (contractions of
heels, legs; Pseudohypertrophy of
calf
muscles)
-
Fatigue
-
Heart disease
People with this disorder experience progressive
muscle weakness of the legs and pelvis, which is
associated with a loss of muscle mass (wasting).
Muscle weakness also occurs in the arms, neck, and
other areas, but not as severely as in the lower
half of the body.
Calf muscles initially enlarge (an attempt by the
body to compensate for loss of muscle strength), but
the enlarged muscle tissue is eventually replaced by
fat
and
connective tissue (pseudohypertrophy).
Muscle contractions occur in the legs and heels,
causing inability to use the muscles because of
shortening of muscle fibers and
fibrosis of connective tissue.
Bones
develop abnormally, causing skeletal deformities of
the chest and other areas.
Cardiomyopathy (damage to the heart) does not
occur as commonly with this disorder as it does with
Duchenne's muscular dystrophy. Cognitive problems
may accompany the disorder, but they are not
inevitable and do not worsen as the disorder
progresses.
Signs and tests
The pattern of symptom development resembles that
of
Duchenne's muscular dystrophy, but with a much
slower rate of progression. Muscle wasting begins in
the legs and pelvis, then progresses to the muscles
of the shoulders and neck, followed by loss of arm
muscles and respiratory muscles. Calf muscle
enlargement (pseudohypertrophy) is quite obvious.
Cardiomyopathy may occur, but the development of
congestive heart failure or
arrhythmias (irregular heartbeats) is rare.
The ability to walk may continue to age
40 or older.
Creatine kinase (CPK) levels may be
elevated.
An
electromyography (EMG) shows that
weakness is caused by destruction of muscle
tissue rather than by damage to
nerves.
Genetic testing
A muscle
biopsy (immunohistochemistry
or
immunoblotting) or genetic test (blood
test) confirms the
diagnosis.
Treatment
There is no known cure for Becker's muscular
dystrophy. Treatment is aimed at control of symptoms
to maximize the quality of life.
Activity is encouraged. Inactivity (such as bed
rest) can worsen the muscle disease.
Physical therapy may be helpful to maintain
muscle strength.
Orthopedic appliances such as braces and
wheelchairs may improve mobility and self-care.
Genetic counseling may be advisable. Sons of a
man with Becker's muscular dystrophy do not develop
the disorder, but daughters will be carriers. The
daughters' sons may develop the disorder.
Immunosuppressant steroids like Prednisone have
been known to help slow the progression of Becker
Muscular Dystrophy. The drug contributes to an
increased production of the protein Utrophin which
closely resembles Dystrophin, the protein that is
defective in BMD.
MY0-029
- Main article: Stamulumab
MYO-029 is an experimental
myostatin inhibiting drug developed by
Wyeth
Pharmaceuticals for the treatment of muscular
dystrophy. Myostatin is a protein that inhibits the
growth of muscle tissue, MYO-029 is a recombinant
human antibody designed to bind and inhibit the
activity of myostatin. A 2005/2006 study, which
included participants afflicted with Becker's, was
completed by Wyeth in Collegeville, PA.
Expectations
and Prognosis
Becker's muscular dystrophy results in slowly
progressive disability. Death usually occurs in the
fifth decade but some patients live to an advanced
age.
Complications
Deformities
Permanent, progressive disability
manifested as decreased mobility or
decreased ability to care for self
Mental impairment
Cardiomyopathy
Noncompaction Cardiomyopathy
Pneumonia or other respiratory
infections
Respiratory failure
Quality of Life
The quality of life for patients with Becker's
muscular dystrophy need not be impacted by the
symptoms of the disorder. With assisting devices,
independence can be maintained indefinitely. People
affected by Becker's muscular dystrophy can still
drive, work, own businesses, and maintain active
lifestyles. |
