Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Conventional MRI has a major
role in the recently developed diagnostic criteria for MS, because
of its exquisite sensitivity for detecting MS lesions and their
changes over time. Conventional MRI lesions are seen as brain (and
spinal cord) multiple foci of various size, irregular shape, and
asymmetric distribution of white matter hyperintensity on
T2-weighted
images. Abnormalities seen on T2-weighted images may reflect edema,
demyelination, remyelination, gliosis, or axonal loss, with a lack
of pathological specificity. A subset of these lesions appear as
hypointense on T1-weighted images, probably more specifically
representing areas of axonal loss and severe matrix destruction. On
post-gadolinium T1-weighted images, some MS lesions can appear
hyperintense, reflecting intense inflammatory activity and
mononuclear cell infiltration.
Despite the sensitivity of conventional MRI for detecting MS
lesions, it does have some important limitations. First, there is
low pathological specificity of the abnormalities seen on
conventional MRI scans.
Second, there is the inability of conventional MRI
metrics to detect and quantify the extent of damage in
normal-appearing brain tissues, which are known to be
involved in the pathological process.
These limitations probably result in the limited
correlation that is found to exist between the conventional MRI
metrics and patients’ clinical status in MS.
These inherent limitations of conventional MRI have prompted the
development and application of modern quantitative MR techniques
such as 1H-MRS, magnetization transfer (MT) MRI, diffusion-weighted
and functional MRI (fMRI) to the study of MS.
1H-MRS
In the last decade, a great number of 1H-MRS studies
have provided in vivo accurate chemical–pathological
characterization of MR-visible lesions and normal
appearing brain tissues in MS brains. In demyelinating
lesions large enough to allow spectra to be acquired
without substantial partial volume effects, 1H-MRS at
both short and long echo times reveals increases in Cho
and sometimes lactate, resonance intensities from the
early phases of the pathological process. Changes in the
resonance intensity of Cho can be interpreted as a
measure of increases in the steady-state levels of
membrane phospholipids released during active myelin
breakdown. Increases in Lac may reflect primarily the
metabolism of inflammatory cells. In large, acute
demyelinating lesions decreases of Cr can also be seen.
Short echo time spectra give evidence for transient
increases in visible lipids (released during myelin
breakdown), and more stable increases in mI. These
changes are consistently accompanied by substantial
decreases in NAA, interpreted as a measure of axonal
injury reflecting metabolic or structural changes.
Recently, glutamate levels were found to be elevated in
acute lesions suggesting a link between axonal injury in
active lesions and glutamate excitotoxicity.
After the acute phase and over a period of days to
weeks, there is a progressive return of raised Lac
resonance intensities to normal levels in focal lesions.
Cr also returns to normal within a few days, or may show
small residual increases, presumably related to gliosis.
Persistent increases in mI signals in chronic lesions
may be related to microglial proliferation. Resonance
intensities of Cho and lipids typically return to normal
over months.
The signal intensity of NAA may remain decreased or show
partial recovery, starting soon after the acute phase
and lasting for several months. The recovery of NAA may
be related in various proportions to reversible
metabolic changes in neuronal mitochondria, the
resolution of edema, or changes in the relative partial
volume of neuronal processes.
Initial 1H-MRS studies were focused mainly on
MRI-defined lesions. However, more recent studies
exploiting the greater coverage and resolution of
1H-MRSI have shown that metabolic abnormalities in MS
patients are not restricted to lesions, but are present
both adjacent to and distant from the lesions.
The NAA decreases found in the normal-appearing white
matter are usually attributed to axonal damage, and,
although they can be present at early disease stages,
are more pronounced in advanced disease stages. The
extent of this NAA reduction decreases with the distance
from the core of a lesion, consistent with the notion
that the diffuse changes are at least in part related to
dying back of axons transected within plaques. However,
decreased levels of NAA also occur without obvious
relation to T2-visible lesions.
Recent 1H-MRS studies have focused on gray matter
metabolic changes in MS patients, supporting the notion
that the contribution of gray matter pathology is
substantial in MS. It has been found that cortical
decreases in NAA might be small or absent early, but
seem to be considerable in patients with progressive
disease. In contrast, subcortical gray matter decreases
in NAA seem to be more consistently found from early
stages. In some studies, 1H-MRS and histopathological
methods have been used in parallel and the amount of ex
vivo total loss of thalamic neurons was comparable to
the in vivo NAA decrease.
A number of spectroscopic studies have demonstrated
highly significant correlations between NAA/Cr and
clinical disability in patients with isolated acute
demyelinating lesions, and in patients with established
MS followed through periods of relapse and remission.
Consistent with other evidence of widespread pathology
in MS, a strong correlation also has been found between
NAA/Cr decreases and increases in clinical disability in
normal-appearing WM. Since changes in Cr could
contribute to any changes in NAA/Cr, it has been
suggested that it would be more accurate to interpret
decreases of brain NAA/Cr as markers of a less specific
disturbance in the “cerebral tissue integrity”.
Despite its potential to monitor the temporal evolution
of metabolite changes reflecting tissue integrity in
demyelinating lesions and normal-appearing brain tissue,
the use of 1H-MRS in longitudinal studies to monitoring
the response to drug therapies are uncommon, and its
large-scale use as a primary or secondary endpoint in
clinical trials has not been attempted. However,
recently recommendations for a standardized use 1H-MRS
protocol in MS multicenter clinical studies have been
provided.
A
B
C
D
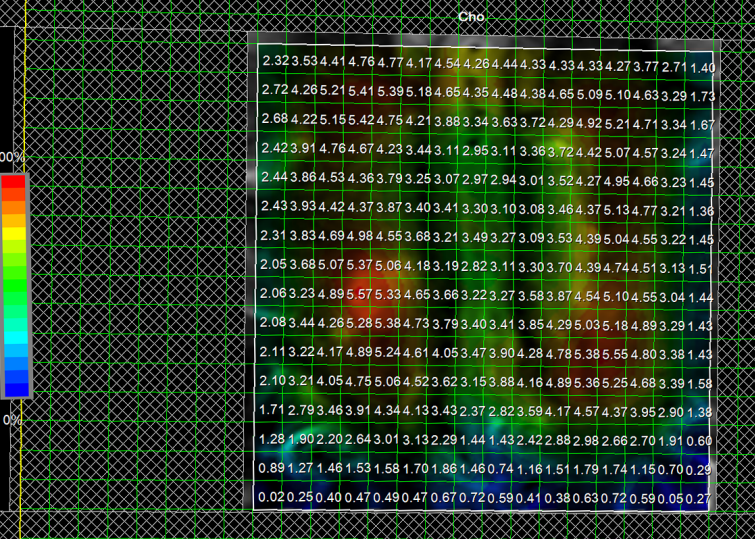
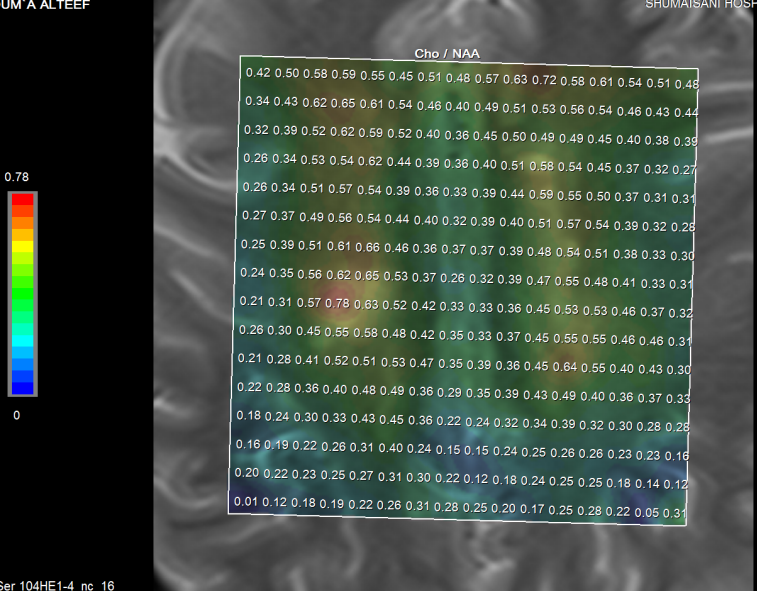
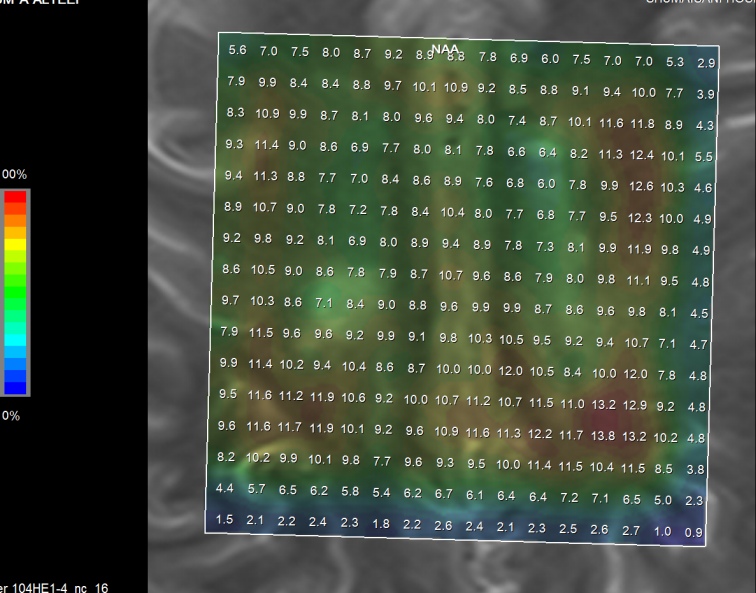
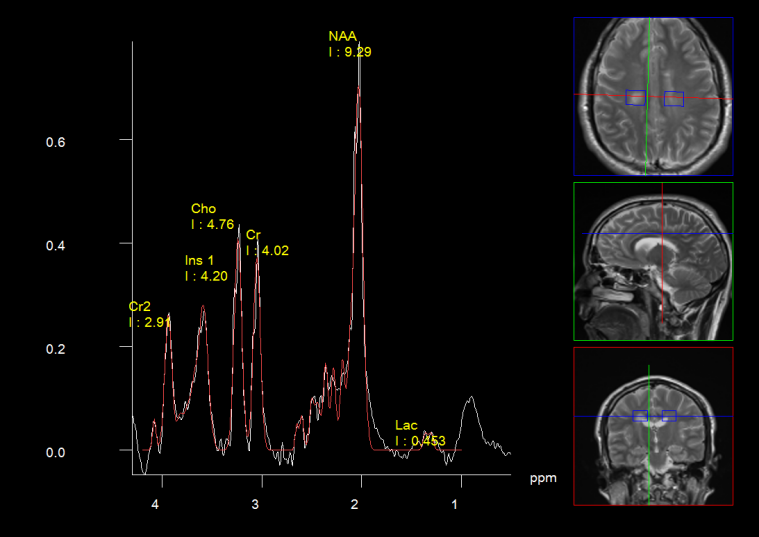
Figure-1: A young patient with second
recent attack of multiple sclerosis, the first was involving
the pons and hemispheres and the second recent involving the
spinal cord at the level of D7-8. Spectroscopic studies were
performed in the old brain lesions with short and medium TE.
Choline, NAA, Cr and Lac were studied in details. The
conclusion from this case was that NAA levels (C) were
distributed evenly in the normal brain and the MS plaques.
Ch (A) was increasing dramatically over the plaques and
still having elevation of the level outside the plaques.
Lactate (D) was decreased all over. The Ch/NAA level (B)
showed elevation in the plaque secondary to the above
obtained results. The studies were performed in Skyra 3
tesla magnetom.
Notice the spinal cord recent lesion,
which at the present time is difficult to perform the
spectroscopic studies at this area, because of technical
limitations (E).
E
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .