Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
23-APRIL-2013 FATMEH ALI AL-NIAAMI 65
YEARS GIANT ANEURYSM LEFT SUPRACLINOID MEDIAL WALL.
Anamnesis
The patient came
to the clinic 16-April-2013 complaining of
headache for 3 years associated with nausea. The
patient underwent left eye surgery for visual
disturbances 18 months ago without improvement. MRI
of the brain done 09-April-2013 showing a huge
mass in the left suprasellar region mostly an
aneurysm of the left supraclinoid with bad
quality MRA, as be the aneurysm involving the
left supraclinoid, left A1 and M1.
On examination: The patient is neurologically
free. She is right handed and have temporal
anopia left visual field. Considering that the performed pictures
showing an aneurysm with high mortality rate and
the good condition of the patient, it was
advised to repeat MRI of better quality and if
the aneurysm of the same description to put the
patient in the wait for progression.
The patient was sent for new
MRI which showed the same aneurysm with good
neck originating just proximal to the
bifurcation of supraclinoid to A1 and M1 distal
to the origin of the anterior choroidal artery.
There are scattered lacunar infarcts in the
vicinity of both cerebral hemispheres.
The patient was admitted to
Jordan hospital and angiography done
18-April-2013 with attempt for embolization,
which was not performed due wide neck of the
aneurysm. Cross circulation is absent from the
right ICA.
Bifrontal approach with left
pterional modification. The bone flap reflected
to the left ear. The frontal sinus was violated
to obtain an approach flush to the base. The
left olfactory tract was bisected and the left
sylvian cistern was opened. The arachnoid
surrounding the left nerve was dissected to gain
better visualization of the left supraclinoid.
The aneurysm was seen fulfilling all sellar
cavity pushing the left optic nerve up. The neck
of the aneurysm was not only wide, but the
supraclinoid was actually part of the lateral
wall of the aneurysm. It was possible to see the
proximal part of the supraclinoid before the
neck and the distal part after the neck and the
A1 and M1 segments. They were full of
calcification. An angled with long blade of
Yasargil Ausculap clip was applied, so as to
create a lumen to the artery from the lateral
wall of the giant aneurysm. After applying the
clip, the created artery is small in diameter
and narrow. Another clip was applied more medial
to the first, away from the created artery and
the first clip was removed. The shape of the
artery regained an acceptable diameter. The
cavity of the closed aneurysm was evacuated by
insulin syringe, the with 20 ml syringe. The
aneurysm collapsed and sellar cavity became
empty, but the wall of the aneurysm was adherent
to the left optic nerve. They were left
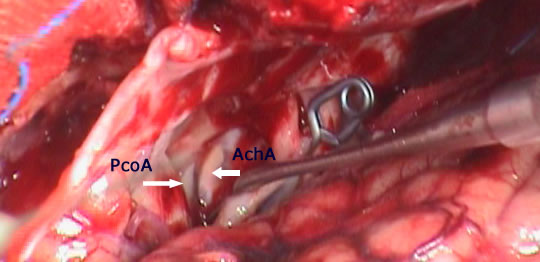
untouched. After evacuation of the aneurysm, it
was possible to see the running under the PcoA
and the AchA left side.
Routine closure of the wound.
Smooth postoperative recovery.
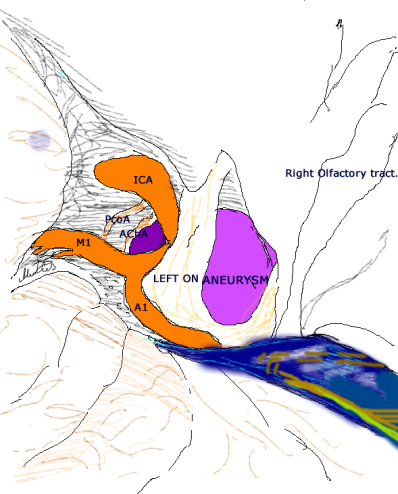
Schematic drawing showing the aneurysm relation before
surgery.
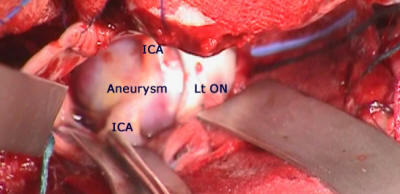
Aneurysm before clipping
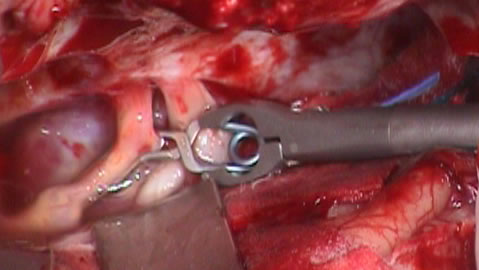
Applying fist clip, the created artery is narrow.
Applying the second clip and the sac evacuated.
Comments
The aneurysm is calcified and application of
clip is full of hazard to fracture of the wall.
For this reason, 2 clip applications were
limited to have the best possible result.
For more information about treating giant
aneurysms please click
here and
here!
Right carotid done 18-April-2013 showing no cross circulation.
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .