Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
04-APRIL-2017 FAWZI SALMAN AFDAL 44
YEARS VERMIAN ANAPLASTIC GLIOMA WITH INVOLVEMENT OF BOTH CEREBELLAR
HEMISPHERES MORE THE RIGHT AND UPPER LEFT.
Anamnesis
The patient was operated 20 days ago in Beirut,
Lebanon through posterior approach and biopsy
was performed, which revealed in 2 separate
histologic verifications that it it was G III
glioma with neuronal differentiation, strong
expression to S-100, GFAP, synaptophysine
positive, Pankeratine and EMA negative. The
patient before this surgery was complaining of
headache and ataxia for 2 months, which improved
slightly after this biopsy and decompression.
MRI of the brain performed 25-March-2017 the
tumor occupying the vermis, reaching the
tentorium in the left side and invading both
cerebellar hemispheres more the right. It is the
same as before the surgery as seen by MRI
performed 02-March-2017. The patient has
congenital deformity of the left foot with burn
below the left knee since childhood.
On examination, the patient is limping with
ataxic gait, which he tells that it is better
than before the first surgery. He is walking
with wide based steppage. Romberg relatively
acceptable. There is no nystagmus and otherwise
neurologically free. The incision in back of the
neck is not midline and shifting to the right
side in the upper part.
he patient was sent for investigations and MRI
of the brain with contrast, MRA of the brain and
carotids, MRV brain, posterior fossa protocol,
SWI, spectroscopy of the tumor and fibertraking
were requested and performed the same day, which
revealed the tumor borders and the malignant
nature of the tumor with high choline levels,
ruling out the hematoma inside the 4th
ventricle. There is collection of fluid around
the bony flap which is pushed slight backward.
The left transverse sinus is not seen in MRV.
In setting position, the
wound was opened and the skin flap slightly
extended up to the left. The bone flap was
hanging free and it was removed and kept. The
dural incision was refreshed and reflected up to
see the infratentorial space and extended down
to see below the tonsils. The tumor was attacked
from above and several pieces sent for permanent
histologic studies. Step wise resection of the
tumor until the floor of the 4th ventricle was
seen from the calamis scriptorius below and the
aqueduct of Sylvius above. Practical resection
of the vermis was achieved with preservation of
the linqula and central lobule above and the
tonsils and tela choroidea below . The patient
was sent for MRI and the resection showed
remnants of the edematous adjacent part of the
right cerebellar hemisphere. MRI spectroscopy
ruled out presence of any active parts of the
resected tumor. That part at the right brachium
pontis was removed and strict hemostasis was
achieved. Routine closure of the
wound.
Smooth postoperative
recovery. The patient responding to verbal
command and moving four limbs. Sent to ICU for
24 hour observation.
Follow Up
The final histologic result was high grade
astrocytoma. The patient walking without aid
07-April-2017, without nystagmus, nor neurologic
deficit.
The patient came 19-January-2020 for follow up
and MRI performed 05-December-2019 showing
complete resolution of the tumor.
Comments
The patient has high grade glioma and
radical resection must be attempted as far as possible to
give the patient a longer period for other treatment
modalities .
Anatomical landmarks must guide the
surgeon about the limits of resection, aided with
intraoperative MRI with spectroscopy to confirm the degree
of resection.
So as to avoid catastrophic postoperative
events, the surgeon must respect the brain stem and the
medulla and in this case the angle between the right
brachium pontis and the right upper corner of the 4th
ventricle.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
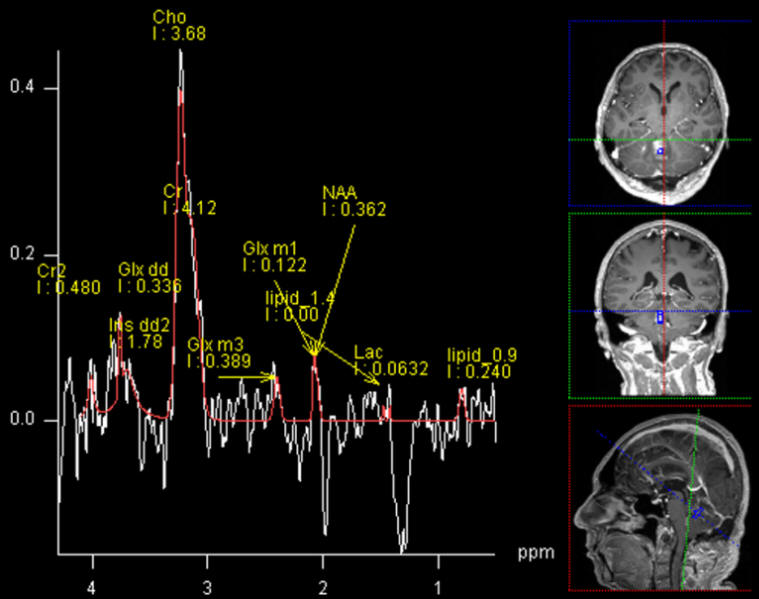
High Choline and low NAA inside the tumor denoting malignant nature
of the mass.
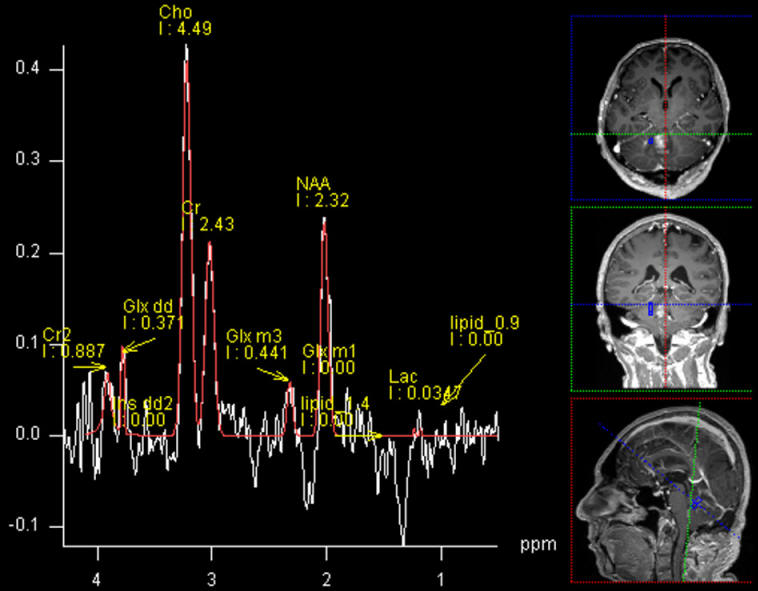
High Choline and low NAA at the right border of the mass confirming
its involvement in the malignant process.
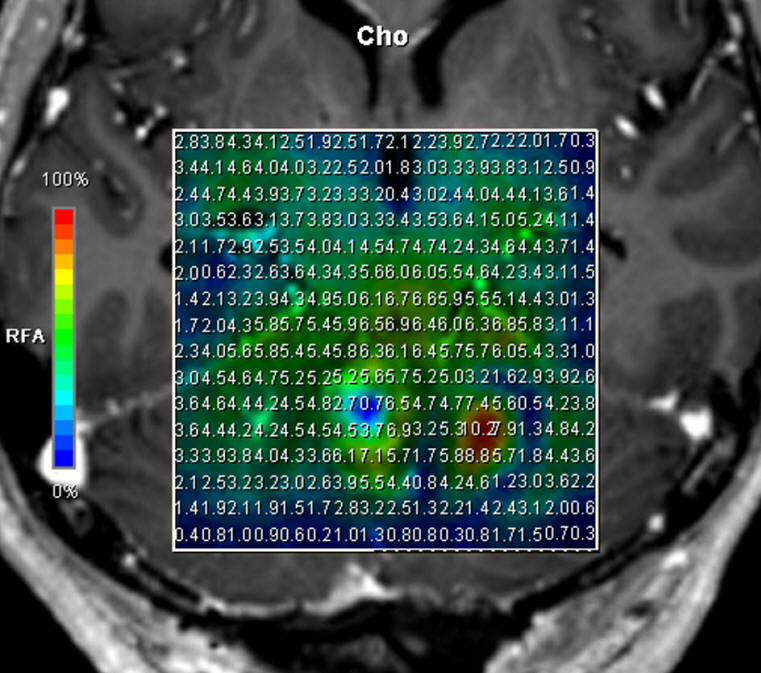
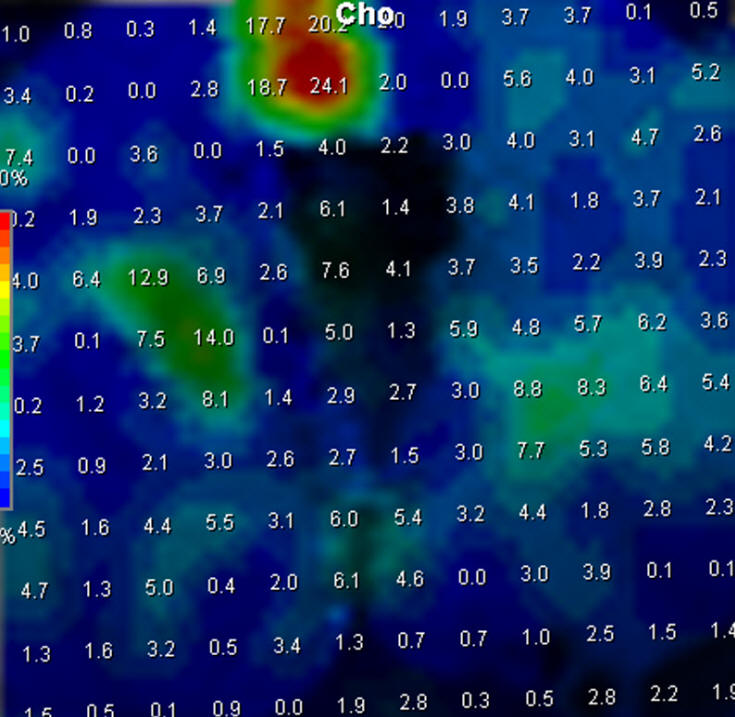
Choline distribution of tumor confirming also the involvement of the
left border of the tumor with left cerebellar hemisphere.
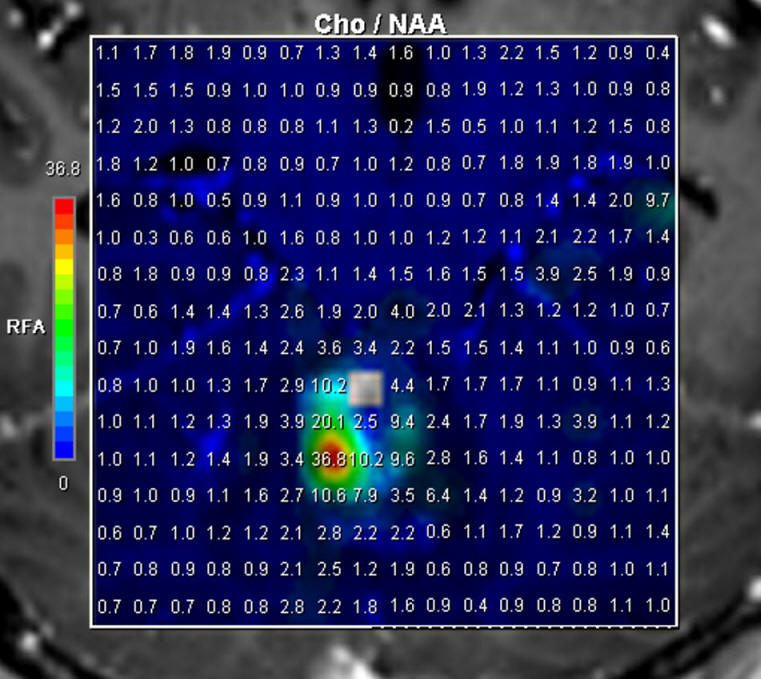
Choline/NAA ratio showing the more active part of the tumor.
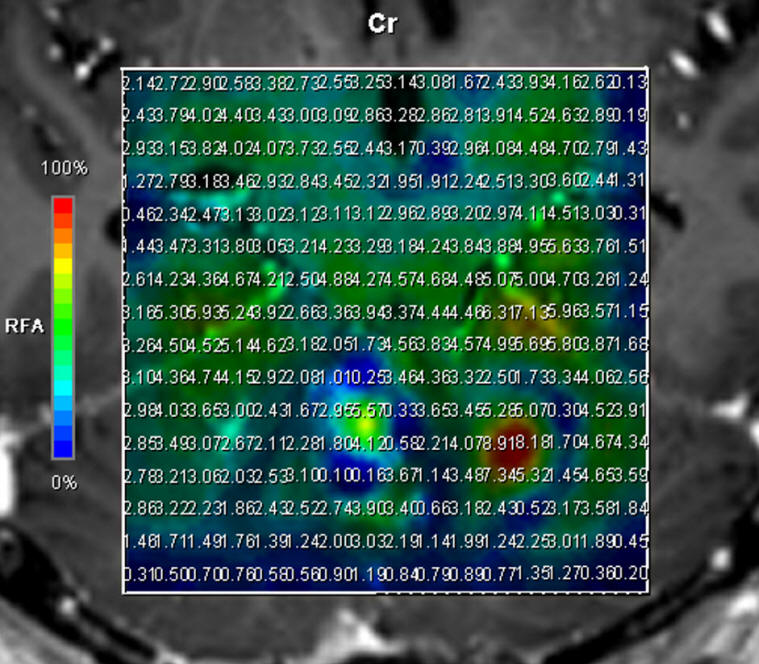
Creatinine distribution which is low in the active place of the
tumor.
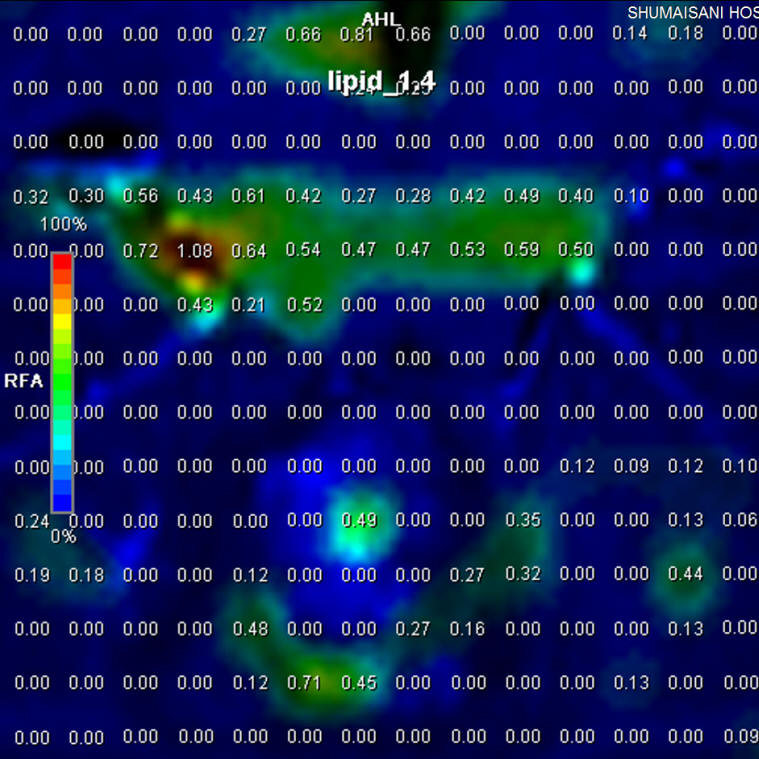
Low lipid inside and around the tumor ruling out lymphoma nature of
the tumor.
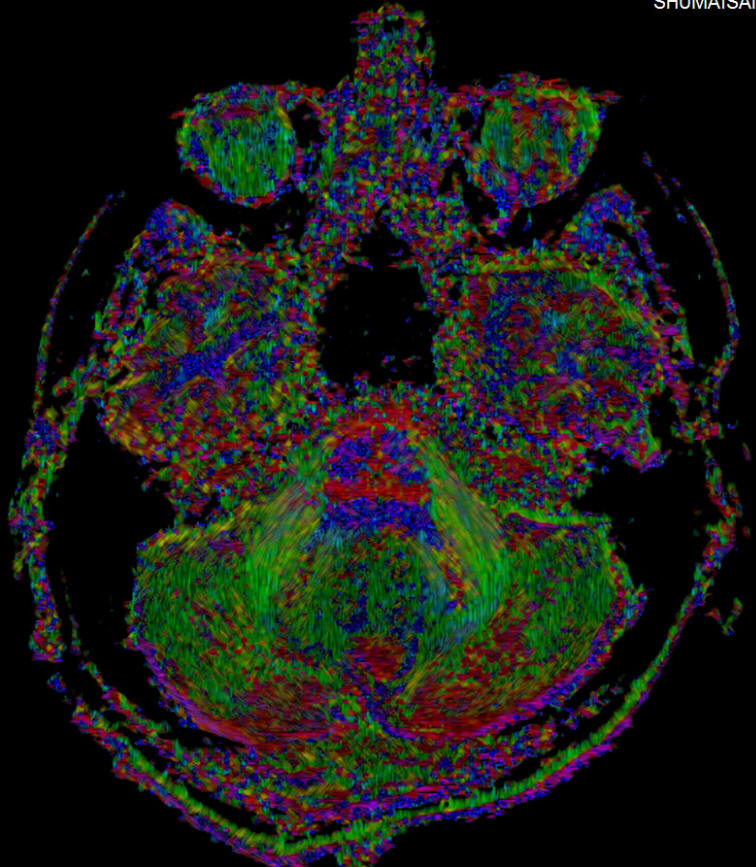
Diffusion tensor showing the tumor with the surrounding fibers
pushed aside.
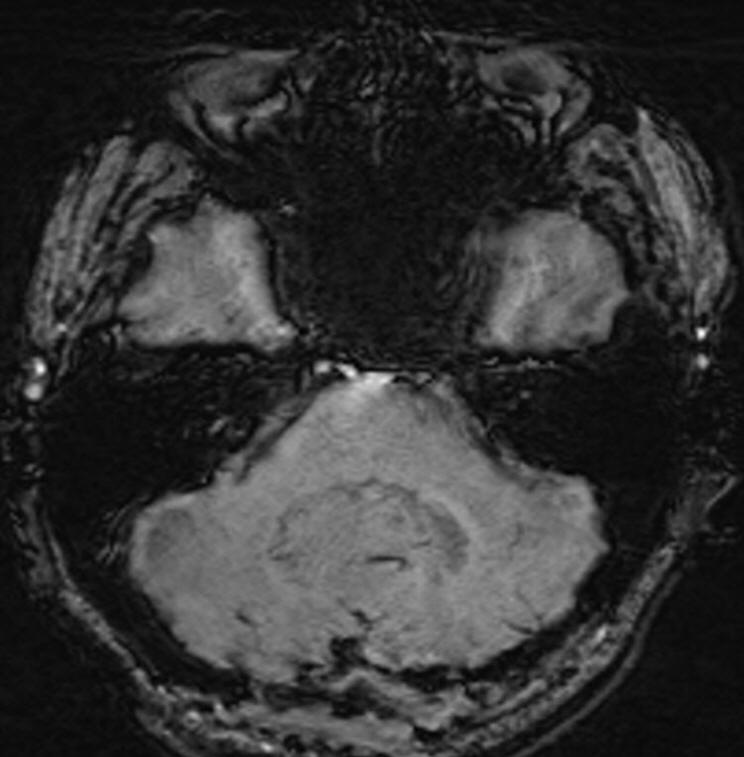
SWI ruling out hematoma nature of the lesion
MR Spectroscopy done during surgery confirming that no residual left
after total resection of the tumor. The upper red part is an
artifact not related tumor area.
Check MRI performed 05-December-2019 showing complete resolution of
the tumor.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .