are neoplasms of the paraganglia. The
paraganglia are small aggregates of cells derived from embryonic neuroepithelium
that are distributed throughout the human body in close association with the
autonomic nervous system. Historically, the paraganglia have been divided into
chromaffin and nonchromaffin subtypes. The carotid bodies are the largest and
best known of the nonchromaffin paraganglia, and along with paraganglia of the
temporal bone, are the most frequent source of paragangliomas encountered by the
neurosurgeon.
Paragangliomas of the carotid body and temporal bone are slowly growing
hypervascular tumors that originate at the carotid bifurcation and in the
temporal bone, respectively. Patients with carotid body paragangliomas typically
present with a painless mass at the angle of the jaw, while those with a
temporal bone paraganglioma usually present with gradual hearing loss and
unilateral pulsatile tinnitus. With larger lesions of either type, multiple
lower cranial nerve palsies are common, and 1 to 3 percent of these tumors
produce catecholamines that may give rise to additional symptoms. Although
paragangliomas haw a predominantly benign appearance histologically, they are
invasive locally and, rarely, can metastasize. They can occur in multiple
locations simultaneously, and at least some seem to be inherited. Multiplanar
computed tomography (CT) or magnetic resonance imaging (MRI) is usually
sufficient for making this diagnosis: therefore, angiography is usually reserved
for outlining the blood supply to lesions that will be treated by embolization
or surgical resection. Complete surgical excision is now possible for most
carotid body and temporal bone paragangliomas and should be the goal for most
patients. Radiation therapy, however, may be an appropriate and effective
therapy for some patients.
Paraganglia: Structure and Function
Since their discovery, the structure and
function of the carotid and temporal paraganglia have been debated. Naturally,
this has led to an unfortunate proliferation of confusing synonyms being applied
to these structures. More recently, however, the role of these structures as
chemoreceptors in a diffuse neuroendocrine system has been revealed. This system
incorporates several organs that contain peptide-producing cells derived from
neuroepithelium that are characterized by amine precursor uptake and
decarboxylation (APUD).
Anatomy
The carotid body is a vascular reddish brown
structure, about the size of a grain of rice, located within the adventitia
posteromedial to the bifurcation of the common carotid artery (CCA). Blood
reaches the carotid body via a fibrovascular bundle, the ligament of Mayer, that
runs from the posterior surface of the CCA to the inferior portion of the
carotid body and supplies the normal carotid body with more blood by weight than
the brain.
The carotid body is innervated by the
intercarotid plexus and the carotid branch of the glossopharyngeal nerve, also
called the carotid sinus nerve or the nerve of Hering. Both receive
contributions from the glossopharyngeal and vagus nerves and from the superior
cervical sympathetic ganglion. Although the major innervation of the carotid
body is sensory, efferent innervation for vasomotor tone control and inhibitory
feedback mechanisms has also been proposed.
The temporal bone paraganglia are smaller
ovoid masses located in various regions of the temporal bones. These bodies do
not have a precise anatomic location but are always found in association with
the nerves of Arnold and Jacobson. In 88 temporal bones from +l patients. Guild
found 248 temporal bone paraganglia. Most temporal bones had at least one
paraganglia while some had as many as 12. Most of the temporal bone paraganglia
( 135 ) were found along the course of the tympanic branch of the
glossopharyngeal nerve (Jacobson' s nerve) at its origin (14), in the adventitia
of the jugular bulb (37), in the tympanic canaliculus, on the promontory (27),
and distally along the lesser petrosal nerve 13. Fewer ( 113) were found in
association with the auricular branch of the vagus nerve (Arnold's nerve) which
runs a variable course. Most of the temporal bone paraganglia found along this
nerve were located within the jugular fossa (81): the remainder were distributed
distally along the mastoid canaliculi between the jugular fossa and the
descending part of the facial canal (19), within the descending facial canal
(7), or accompanying an aberrant branch of Arnold's nerve that passed external
to the skull base between the jugular fossa and the stylomastoid foramen (6).
The sex, race, or side studied appears to make no difference in the number or
position of these bodies. The number of paraganglia seems to increase until the
fourth decade of life and then to decline.
Both Arnold's and Jacobson's nerves are
accompanied by branches of the inferior tympanic branch of the ascending
pharyngeal artery. This vessel supplies blood to the normal temporal bone
paraganglia. Neoplasms may recruit additional blood supply from a variety of
other sources, however, The temporal bone paraganglia are innervated by Arnold's
and Jacobson's nerves along with some branches from the superior cervical
sympathetic ganglion.
Histology
The carotid and temporal paraganglia are
indistinguishable histologically. Wide bands of cartilaginous connective tissue
divide the parenchyma into lobules. Each lobule is nourished by a single
arteriole and is divided into three to six cell nests. Each of these cell nests,
called glomeruli of Zellballen, contains 20 to 40 cells of various types that
are surrounded by a sinusoidal vascular network.
The parenchyma of the paraganglia consists of
two primary cell types. These are best called type I and type II cells. Type I
cells are more common and are typically round with indistinct cell borders. Type
I cells may be further divided into light, dark, and pyknotic subtypes that may
have different functions. The role of type I cells. however, remains unknown.
Because they store a variety of biologically active amines, it is tempting to
postulate that these substances are released in response to chemical changes in
the blood. On the other hand, these chemicals could modulate other
chemoreceptive nerve endings. Similarly. type I cells could act as interneurons.
Type II cells are smaller and irregularly shaped. They are situated between the
type I cells and the surrounding vascular sinusoids. These cells may act as
glial-like sheaths for the type I cells.
Paragangliomas
Pathology
Operative specimens from carotid body or
temporal bone paragangliomas are generally indistinguishable. Smaller tumors may
be grooved by the carotid arteries while larger ones may have vessels imbedded
in the sample. These tumors tend to be smooth and well circumscribed. They have
a rubbery consistency, and the cut surface is usually homogeneous except for
some occasional areas of necrosis, fibrosis, or hemorrhage.
Although paragangliomas of the carotid body
and temporal bone are generally regarded as benign. they are histologically
invasive and can rnetastasize. Typically, rates of malignancy of 3 percent for
temporal bone tumors and 12 percent for carotid body tumors are quoted, although
some reports quote rates as high as 30 to 50 percent. The definition of
malignancy for paragangliomas is difficult to establish, however. These tumors
tend to develop spontaneously in multiple locations and to recur frequently. On
the other hand, paragangliomas may grow very slowly and often lack histologic
changes characteristic of other malignant tumors. Only relatively recently was a
reduction in the proportion of type II cells and a poorer staining of type I
cells for S-100 and glial fibrillary acidic protein (GFAP) reported to be
correlated with an increased tumor grade. Finally, although patients with
metastatic paragangliomas may quickly succumb, their prognosis is completely
unpredictable, and some patients with multiple metastatic lesions survive for
several decades.
The nonchromaffin paragangliomas also have a
familial tendency. An analysis of 15 pedigrees by van der Mey and colleagues
found that paragangliomas were inherited in an autosomal dominant fashion but
were transmitted almost exclusively by males. For example, an affected father
resulted in 28 percent (23/82) of descendants (11 males and 12 females) being
affected, while in families with an affected mother, the disease was reported in
only one descendant with a questionable diagnosis. This pattern of inheritance
is best explained by a hypothesis of genomic imprinting by which a maternally
derived mutant gene that leads to the development of a paraganglioma is
inactivated during oogenesis only to be reactivated during spermatogenesis in a
subsequent generation. Overall, half the patients in this series had a positive
family history.
As could be expected, a positive family
history also places a patient at increased risk for developing a second primary
paraganglioma. In this circumstance, up to one-third of patients will have a
second paraganglioma. Multicentric paragangliomas, however, are discovered in as
many as 10 percent of patients without a significant family medical history. The
onset of these multicentric tumors may be synchronous or delayed by several
decades. Bilateral carotid body tumors are the most frequently encountered
example. These are followed in frequency by the combination of a carotid body
tumor and a temporal bone tumor and then other combinations. Plurifocal tumors
can occur in 3 to 5 percent of patients.
Clinical Presentation
Carotid Body Paragangliomas
Carotid body tumors are the second most
frequently encountered nonchromaffin paragangliomas after temporal bone
paragangliomas. More than 1000 cases have now been reported in the literature.
These tumors usually present in patients in the fourth, fifth, or sixth decade
of life, although reported cases range in age from 3 months to 89 years. An
average tumor size is 4.5 x 3.5 x 3 cm, with the largest tumors exceeding 15 cm
in diameter and weighing almost 200 g. There may be an increased incidence of
these tumors in high-altitude dwellers, and although some reports show a female
predominance greater than 5:1, carotid body tumors are less sex-specific than
temporal bone paragangliomas.
Classically, carotid body tumors grow with
progressive involvement of the internal and external carotid arteries, usually
without constricting the arterial lumens. These lesions can extend into the base
of the skull through a foramen or by bony erosion. Alternatively, they may grow
medially or laterally and into the peripharyngeal space or inferiorly to invade
the clavicle. The clinical manifestations of these tumors generally can be
ascertained from these characteristic growth patterns. The widely accepted
Shamblin classification system of carotid body tumors is primarily used for
staging purposes, but also allows a comparison between different therapeutic
modalities.
Patients with carotid body tumors typically
present with a painless mass at the angle of the jaw that may be partially
covered by the sternocliedomastoid muscle. Although many other possibilities
exist in the differential diagnosis of such lesions (Table-1 ). Classically, the
mass from a carotid body tumor is mobile laterally, but is restricted from
vertical movement because of its attachment to the bifurcation of the CCA. These
vascular tumors may transmit pulsations from the nearby carotid arteries or may
be pulsatile inherently. The mass may shrink and re-expand spontaneously or with
digital compression, and infrequently a bruit may also be heard over the mass.
Larger tumors may produce a pharyngeal bulge that may displace or erode the
tonsil, soft palate or uvula. In these instances, patients may present with
spontaneous oropharyngeal bleeding. Occasionally, however, these tumors are
discovered incidentally at angiography, surgery or autopsy.
TABLE-1 Differential Diagnosis of Carotid Body
Paragangliomas
Lymphadenitis
Fibroma. lipoma. hemangioma.
Lymphoma
dermoid. teratoma
Branchial cleft cyst
Aneurysm
Lymph node metastases
Giant cell arteritis
Lateral aberrant thyroid
Hematoma
Vagal or sympathetic neurogenic
tumors
Carotid stenosis with poststenotic
dilatation
Salivary gland
tumors
Carotid calcification
An invasion of surrounding neural
structures in the neck can result in a variety of additional sequelae. At
the time of diagnosis, cranial nerve palsies are usually present in less
than 10 percent of patients. The vagus and hypoglossal nerves are most
frequently involved, and this usually leads to dysphagia or hoarseness.
Cranial nerves V and VII may also be involved, however. In addition,
infiltration of the cervical or brachial plexus may result in the mass being
painful or tender, while involvement of the cervical sympathetic chain can
produce a Horner's syndrome. The distant effects of these tumors are varied
and remain for the most part unexplained. Perhaps the best example of this
phenomenon is the carotid sinus syndrome. This syndrome of bradycardia,
hypotension, and a loss of consciousness may occur spontaneously or
secondary to head movement or direct pressure on the tumor in some patients
with carotid body paragangliomas. Additional reports of such systemic
abnormalities that have resolved after tumor excision include alterations in
gut motility with emesis on manipulation of the tumor, extensive skin
alterations. constitutional symptoms such as weight loss and fever and
even one case of membranous glornerulonephritis. Finally. while
catecholamine production is exceedingly rare for extra-adrenal
paragangliomas, a few patients with these tumors may present with a variety
of symptoms or signs secondary to catecholamine production.
Norepinephrine is the usual product and hypertension is the most frequent
finding. Although only a handful of such cases have been reported in the
literature, being unaware of functional tumors can have disastrous
consequences during embolization or surgery. Therefore, patients with
suspicious findings should have free norepinephrine, epinephrine. and
3,4-dihydroxyphenylglycol measured in a 24-h urine collection. If these
tests confirm the presence of such a tumor then the patient should undergo
an appropriate adrenergic blockade prior to embolization or surgery (Table
-2).
TABLE-2 Treatment Guidelines for
Adrenergic Blockade a-Adrenergic Blockade
α-Adrenergic
Blockade
At least 2 weeks before surgery, establish
adequate blockade in all patients with norepinephrine- and
epinephrine-secreting tumors.
Begin with phenoxybenzamine, 10 mg twice a
day: increase by 10 mg/day at 3-day intervals: 10-20 mg 3 times a day
usually suffices.
Maintain patient on
generous salt diet to expand blood volume.
β-Adrenergic
Blockade
Indicated in patients with a heart rate
greater than 110 beats/min. history of arrhythmias or persistent ventricular
extrasystoles. or predominantly epinephrine-secreting tumor: also in
patients with pulse rate greater than 110 beats/min after initiation of
phenoxybenzamine therapy.
For most patients. begin with propranolol.
not to exceed 10 mg 3 times a day: 30-60 rug/day usually suffices. For
patients with history of bronchospastic disease use low-dose metoprolol or
equivalent cardioselective beta-blocker.
Do not initiate
β-adrenergic blockade
until α-adrenergic blockade is at least partially established.
Temporal Bone Paragangliomas
Temporal bone paragangliomas are the most
frequently encountered benign tumor of the temporal bone, and must be
considered in the differential diagnosis of temporal bone lesions (Table3). Although frequent histologic misinterpretation, difficulties with
nomenclature, and republication of cases make estimates of prevalence
difficult, well over 1000 cases have been reported in the world
literature. These tumors usually present in patients in the fifth decade
of life, although reported cases range in age from 22 months to 85 years
of age. Females with temporal bone paragangliomas outnumber males
approximately 3 : 1 in most large series and ratios of 10: 1 have been
reported. Larger studies also suggest a preference for the left side,
especially in females.
TABLE-3 Differential Diagnosis of
Temporal Bone Paragangliomas
Otitis media
Otosclerosis
Chronic
mastoiditis
Cholesteatoma
Cholesterol granuloma
Eosinophilic
granuloma
Chordoma
Vestibular schwannoma
Meningioma
Metastasis
Aneurysm
Aberrant intrapetrous internal
carotid artery
Idiopathic hemotympanum
Arteriovenous malformation
Prominent jugular bulb
Persistent stapedial artery
Paragangliomas of the temporal bone are
generally divided into those that originate within the middle ear, glomus
tympanicum tumors, and those that originate within the jugular fossa. glomus
jugulare tumors. This latter term, however, is often used to refer to large
tumors where the origin is difficult to determine. The predominance of the
paraganglia within the jugular fossa likely accounts for the increased
frequency of tumors with this origin. Classification systems that have been
developed for temporal bone paragangliomas are used for staging purposes.
surgical planning, and comparison among different therapeutic modalities.
The Glasscock-Jackson (Table-4) and Fisch (Table-5)
classifications are the most widely employed.
TABLE 154-4
Glasscock-Jackson Classification of Temporal Bone Paragangliomas
Type I Small tumor involving the jugular
bulb. middle ear. and mastoid
Type II Tumor extending under internal
auditory canal: might have intracranial extension
Type III Tumor extending into petrous
apex: might haw intracranial extension
Type IV Tumor extending beyond petrous
apex into clivus or infratemporal fossa: might have intracranial extension
TABLE-5 Fisch Classification of
Temporal Bone Paragangliomas
Class A: Tumors limited to the middle ear
cleft
Class B: Tumors limited to the tympanomastoid area without destruction of bone in the infralabyrinthine
compartment
Class C: Tumors extending into and
destroying bone of the infralabyrinthine and apical compartments of the
temporal bone
C1: Tumors destroying the bone of the
jugular foramen and jugular bulb with limited involvement of the vertical
portion of the carotid canal
C2: Tumors destroying the
infralabyrinthine compartment of the temporal bone and invading the vertical
portion of the carotid canal
C3: Tumors involving the infralabyrinthine and apical compartments of the temporal bone with invasion
of the horizontal portion of the carotid canal
Class D: Tumors with intracranial
extension
D1: Tumors with intracranial extension
up to 2 cm in diameter
D2: Tumors with an intracranial extension greater than
2 cm in diameter
D3: Tumors with inoperable intracranial
extension
The symptoms and signs that result from
paraganglia of the temporal bone can be conveniently divided into otologic
and neurological manifestations. Otologic symptoms usually predominate for
both glomus jugulare and glomus tympanicum tumors. Unilateral hearing loss
is the most frequent initial symptom and will be present in most patients.
Typically it is gradual in onset, but an acute onset should not exclude the
diagnosis. Although the hearing loss can be of the conductive type, sensorineural hearing loss is usually present at the time of diagnosis in
most patients. This indicates involvement of the labyrinth or eighth
cranial nerve and a poorer prognosis. Unilateral tinnitus,
synchronous with the pulse, is the second most frequently reported symptom.
Often, this is coincident with an audible bruit and both can be reduced
with neck turning or direct pressure on the tumor. Otoscopic examination
may reveal a gray-red mass in the external auditory canal or a hypervascular
or bulging tympanic membrane. This mass may not be pulsatile on first
inspection, but pulsations usually can be demonstrated by increasing the
pressure within the external auditory canal using a pneumatic otoscope.
Examination with the otoscope can also confirm bleeding from the lesion or
an associated chronic otitis media that may lead to otalgia, meningitis or
brain abscess. Neurological symptoms and signs generally follow otologic
symptoms by several years, but ultimately these tumors produce neurological
symptoms or signs in one-third to two-thirds of patients. These
neurological findings are very important in classifying the stage and
extent of these tumors. Neurological manifestations of these lesions result
from involvement of either the cranial nerves or the brain. Although
temporal bone paragangliomas can lead to a palsy of any adjacent cranial
nerve, the facial nerve is the most commonly involved. The facial nerve may
be affected in the middle ear or by extension of the tumor into the mastoid
or internal acoustic meatus. In a similar way, vertigo may be secondary to
involvement of the labyrinth, or secondary to compression of the eighth
nerve directly. The resultant nystagmus is usually horizontal, but vertical
and rotatory nystagmus have been reported. The lower cranial nerves are also frequently
involved. Patients with glomus jugulare tumors often present with a jugular
foramen syndrome that includes palsies of the ninth, tenth and eleventh
cranial nerves. Greater cranial nerve involvement generally correlates with
increased invasion of the nervous system and a worse prognosis.
Involvement of the central nervous system
generally results from extension of the tumor into the middle or posterior
cranial fossa, especially in the region of the cerebellopontine angle.
Besides additional cranial nerve palsies, this can produce headache,
increased intracranial pressure, cerebellar and long tract signs, or a
Horner's syndrome. Seizures from temporal lobe penetration by a
paraganglioma have been reported, and these tumors have been cited as the
cause of cerebral ischemic events, congestive heart failure, and
subarachnoid hemorrhage. A few patients with these tumors may also present
with a variety of symptoms or signs secondary to catecholamine production
as described above for carotid body tumors.
Radiographic Evaluation
Patients suspected of having a carotid
body or temporal bone paraganglioma should undergo a noninvasive
radiographic study to exclude more common entities and to detect an
additional unsuspected paraganglioma at another location. The initial
radiographic investigation selected depends on the clinical impression.
Patients with a temporal bone paraganglioma thought to be limited to the
middle ear (glomus tvmpanicum should undergo high-resolution, axial and
direct coronal bolus-enhanced CT of the temporal bone and surrounding structures. A small glomus tympanicum tumor will appear as a
contrast-enhancing soft tissue mass on the promontory within the middle ear
cavity. If the bony septum that separates the jugular bulb and
carotid artery from the middle ear is intact, then several vascular
abnormalities within the differential diagnosis can also be excluded.
Furthermore, any tumor present can be considered limited to the middle ear.
This has considerable importance in selecting the appropriate surgical
approach.
Patients thought to have a carotid body
paraganglioma or a temporal bone paraganglioma that extends beyond the
middle ear or that originates next to the jugular bulb (glomus jugulare)
should undergo multiplanar, thin-section, T1- and T2-weighted and
gadolinium diethylenetriaminepenta-acetic acid (DTPA) enhanced MRI.
Paragangliomas have an intermediate signal on T1-weighted and a high signal
on T2-weighted images and enhance intensely. In addition,
paragangliomas greater than 2 cm in size produce a characteristic
salt-and-pepper appearance that results from the fast-flowing blood pools
and large tumor vessels within these lesions. Although this appearance in
the petromastoid region is almost pathognomonic for a temporal bone
paraganglioma, renal and thyroid carcinoma metastases and hemangiomas can
be confused with carotid body paragangliomas in the peripharyngeal space.
Although MRI clearly proves involvement of the carotid arteries and jugular
vein by these lesions, bony landmarks in the skull base are poorly defined
by MR images. and parallel imaging with CT may be necessary.
Cerebral angiography remains the gold
standard for the diagnosis of head and neck paragangliomas, but in
practice, this study is reserved for patients who have larger tumors and who
are scheduled for embolization or resection. The main goal of angiography
in such patients is to delineate the vascular anatomy of the tumor. However, it can also be used to determine
the presence of internal carotid artery invasion and to evaluate for
atherosclerotic disease, patency of the circle of Willis. and the patient's
tolerance of balloon test occlusion. Both external carotid artery (ECA) and
internal carotid artery (lCA) iodinated contrast injections are routinely
employed. If intracranial extension is suspected, vertebrobasilar
angiography will also be necessary.
Paragangliomas have an angiographic
appearance midway between that of a meningioma and that of an arteriovenous
malformation. Early phases show variably sized pathologic vessels around
the tumor site. This is followed by an intense, occasionally inhomogeneous
staining of the tumor. For temporal bone tumors such a tumor blush appears
in the middle ear and may be obscured by the overlying temporal bone. Thus,
subtraction techniques may be necessary. Other findings with temporal bone
paragangliomas may include an increase in the number and size of branches
passing from the ECA to the temporal bone and displacement of vessels
within the middle or posterior cranial compartment. Besides the
characteristic tumor blush in patients with a carotid body tumor, a
characteristic distortion of the carotid bifurcation is also visible on
angiography. The ICA is generally pushed laterally and
posteriorly while the ECA is displaced anteriorly.
Other diagnostic techniques may also be of
value if applied under appropriate circumstances. For example, about half of
all head and neck paragangliomas can be detected using iodine-123 metaiodobenzylguanidine (MIBG) scintigraphy. Most nonchromaffin
paragangliomas show low uptake of this tracer: therefore, single photon
emission computed tomography (SPECT) images are needed to eliminate the
interference created by the normal uptake of tracer in the parotid and submandibular glands. In addition, total body scintigraphy with
123I-MIBG
can be used as a screening tool to detect distant additional primary or
metastatic lesions in patients or their near relatives. Although it is often
speculated that such uptake, especially if intense, suggests a norepinephrineproducing tumor, the uptake of
123I-MIBG can be independent
of catecholamine secretory activity. In lesions that show tracer uptake,
this technique can be used to document the results of therapy or to treat
unresectable lesions by using radiotherapeutic doses of 131I-MIBG. Color
Doppler ultrasound can also be used to demonstrate vascular lesions that
disrupt the carotid bifurcation, but it will not reliably differentiate
between carotid body tumors and other vascular lesions in the area.
Treatment
There are four treatment options for
patients with carotid body or temporal bone paragangliomas. These can be
used alone or in various combinations. The ideal treatment for most
patients is complete surgical excision of the tumor. Endovascular
embolization can be used preoperatively to facilitate such a resection, but
insufficient evidence exists to warrant its isolated use. In patients not
suited for operative therapy, irradiation may be a useful measure for
primary or metastatic disease. Chemotherapy, on the other hand, has been
reserved for patients with systemic metastases and has no proven efficacy
except for a few isolated case reports.
Embolization
Endovascular embolization of carotid body
or temporal bone tumors may reduce operative time and limit blood loss.
This was shown in one representative work by Ward and colleagues who
retrospectively compared six patients with carotid body tumors who underwent
preoperative embolization to ten patients with 11 tumors who did not.
They found a reduction in average operative time from 4.24 h to 1.75 h. The
blood loss was also reduced from 1250 ml to approximately 400 ml. Although
these authors also observed a reduction in operative cranial nerve injuries
in patients who underwent preoperative embolization. they provide no basis
for comparison between the two groups for other important parameters such
as tumor classification or size. Similarly, Murphy and Brackmann reported a
series of patients with temporal bone tumors stratified according to the
Fisch classification system. Eighteen patients underwent preoperative
embolization while 17 patients did not. When patients with tumors from all
classifications were grouped together, embolized patients showed a
significant reduction in operative blood loss from 2769 ml to 1122 ml (p <
0.005) and a reduction in operative time from 7.95 h to 7.04 h (p < 0.005).
However, Murphy and Brackmann could not show a reduction in postoperative
cranial nerve deficits with embolization. In both of the above studies,
however, the embolized patients were always later in the series. Therefore,
these conclusions are confounded by other variables such as an increase in
the experience of the operative team. Although some authorities have not
found preoperative embolization necessary, most now employ this technique
for Shamblin type III carotid body tumors and Fisch type C2.3 or D temporal
bone tumors. Embolization usually takes place immediately following the
diagnostic angiogram and is then followed soon after by surgery to prevent
the recognized phenomena of collateral vessel formation and recanalization.
Temporal bone paragangliomas may be
composed of up to four hemodynamically isolated compartments. Each of
these compartments is primarily supplied by different branches of the
ECA. Therefore, superselective catheterization of specific branches of the
ECA is necessary for complete embolization of a multicompartmental tumor.
Blood supply from the internal carotid and vertebral arteries can be shown
for some anteriorly located tumors that may be supplied by the caroticotympanic branch of the ICA. Large tumors with extradural
intracranial extension may also be supplied by clival and cavernous branches
of the ICA. The intradural component of Fisch type D, tumors is always
supplied by parenchymal branches from the vertebrobasilar system, usually
the posterior inferior cerebellar artery at the level of the jugular
foramen and the anterior inferior cerebellar artery in the
cerebellopontine angle.
Complete devascularization of Fisch type C
and at least partial devascularization of type D tumors can usually be
achicved. Tumors with an anterior component supplied by the caroticotympanic artery can be embolized completely only if this artery
can be selectively catheterized and there is no evidence of contrast reflux
into the ICA. Otherwise tumors with significant ICA blood supply can only be
embolized by balloon occlusion of the petrous ICA provided the patient has
tolerated temporary balloon occlusion and hypotensive testing before
embolization. The intradural portion of type D tumors is supplied by the
vertebrobasilar system and cannot be embolized safely.
Preoperative embolization of temporal bone
paragangliomas is usually followed by a fever and transient ear pain. This
procedure may also be complicated by wound healing problems, cerebral
ischemia, and lower cranial nerve palsies. Ischemic cerebral events are most
likely to occur if arterial anastomoses exist between the branches of the
ECA supplying the tumor and the ICA or vertebrobasilar arterial system. Such anastomoses, present in as many as one-third of patients, are not a
contraindication to embolization, but special techniques such as temporary
occlusion of the anastomotic artery or the use of embolic particles larger
than the anastomotic artery must be employed. Similarly, permanent new
cranial nerve palsies may develop if nonabsorbable embolization material is
injected into the neuromeningeal branch of the ascending pharyngeal artery
that supplies cranial nerves IX through XII or the stylomastoid and middle
meningeal arteries that supply blood to cranial nerve VII. Absorbable
materials such as Gelfoam may still produce cranial nerve palsies, but these are
usually transient.
Preoperative embolization of carotid
body tumors follows the same basic principles as outlined above for
temporal bone paragangliomas. Most carotid body tumors are also multicompartmental, with the bulk of the blood supply coming from the
ascending cervical artery and the musculospinal branch of the ascending
pharyngeal artery. The tumor may also be supplied by the facial,
lingual, thyroid, posterior auricular, occipital, and deep cervical
arteries. The artery of the carotid body that also supplies these tumors
cannot usually be identified on angiography, and therefore cannot be embolized.
Radiation Therapy
Opinions vary on the value of
radiation therapy in the treatment of the paragangliomas of the carotid
body and temporal bone. The debate centers on the radiosensitivity of
these tumors. Histologically, radiation results in edema, fibrosis, hemosiderin pigmentation and degeneration of the vessel walls with
intimal proliferation leading to partial obliteration and thrombosis. It seems not to affect the cellular elements of the paragangliomas,
however, with most tumors retaining many areas that appear viable.
Unfortunately. there are no generally
accepted criteria for successful radiation therapy of these lesions.
While some authors claim that all patients treated with radiation
therapy obtain symptomatic relief, few report significant regression of
the tumor mass and no evidence exists to show that local irradiation
decreases the risk of developing metastases. To evaluate the results of
radiation therapy for these lesions. Springate and colleagues reviewed
the literature on the treatment of temporal body paragangliomas
published from 1965 to 1988. In this review, all patients without
evidence of disease progression on clinical or radiographic examination
were considered to have been treated successfully. Using this
definition, they averaged the cases reported in the literature and
found success rates of 86. 90. and 93 percent for surgery alone.
irradiation with or without surgery, and irradiation alone,
respectively. While such a comparison is used to advocate radiation
therapy as a primary treatment for head and neck paragangliomas, it
fails to recognize that the goal of surgical therapy, that is,
eradication of disease, is different from the goal of radiation therapy,
which is limitation of disease progression. As a result, no valid
comparison between radiation and surgical therapy exists in the
literature.
Despite these concerns, radiation
therapy for patients with carotid body or temporal bone paragangliomas
leads initially to symptomatic relief in most patients. Neurological
deficits, however, are rarely relieved and may progress after
irradiation. For example, Cummings and colleagues reported on a series
of 45 patients who received radiation therapy for temporal bone
paragangliomas. In this group, most patients were relieved of tinnitus
(30/38), pain (8/8), and vertigo (5/5), although this was sometimes
delayed for several months. Furthermore, these symptoms recurred in
only three patients during a follow-up period that ranged from 3 to 23
years. In contrast, only two patients had significant relief of cranial
nerve deficits. Similarly, Valdagni and Amichetti reported on 13 carotid
body tumors in seven patients followed from 1 to 19 years after
Irradiation. While no patient in this series was considered to have
progressive disease, only three tumors displayed regression and only
seven patients had symptomatic relief.
Complications secondary to radiation
therapy for temporal bone paragangliomas are generally more severe than
those encountered during the treatment of carotid body tumors. The most
serious sequelae from radiation of temporal bone paragangliomas include
brain and temporal bone necrosis that may be life-threatening. This
complication is reported in one or two patients in most series, for an
average of slightly less than 4 percent. These patients have almost
always received more than the standard 35005000 rad megavoltage dose
given via a homolateral wedge pair technique over 3 to 5 weeks in most
centers. Other less severe complications associated with temporal body
paraganglioma irradiation include protracted otorrhea or otitis,
vertigo, ataxia and external auditory canal stenosis. Although the
complications associated with carotid body tumors are infrequent and
generally trivial, radiation therapy may result in delayed hemiplegia, postradiation stricture of the larynx, and
radionecrosis of the carotid artery and mandible. Such radiation will
also complicate subsequent surgery. Therefore, radiation therapy as a
treatment should be limited to patients who are elderly and
asymptomatic, who have undergone incomplete resection, who refuse
surgery, or who develop recurrent or metastatic lesions. Patients who
have bilateral paragangliomas with severe cranial nerve deficits,
especially of the glossopharyngeal and vagus nerve on one side secondary
to tumor progression or surgical excision, should also be considered for
radiation therapy. Experience is now accumulating with
the radiosurgical treatment of temporal bone paragangliomas. Time will
tell whether this approach is better than conventional radiotherapy.
Surgical Therapy:
Carotid Body
Paragangliomas
Complete surgical excision remains the
preferred treatment for most patients with carotid body tumors. This is
especially true for tumors that display aggressive or invasive growth
locally. Small tumors, tumors that interfere with normal function and
tumors in young people should also undergo surgical removal. With
advanced techniques, including intraoperative cerebral blood flow and
electroencephalographic monitoring; lCA shunting, grafting or
reconstruction; and mobilization of the parotid gland: nearly all
carotid body tumors can be resected completely with small risk of stroke
or death. For example, among 30 cervical paragangliomas, mostly Shamblin
type II carotid body tumors, resected between 1976 and 1986, Hallett and
colleagues reported only one stroke and no deaths.
Postoperative cranial nerve deficits
and arterial injury, however, have remained a significant problem.
While only 10 percent of patients in the above series were found to have
cranial nerve deficits preoperatively, this number increased to 40
percent postoperatively. Fortunately, these deficits were transient
in one-half of these patients. The most frequently affected nerves were
the hypoglossal nerve and the vagus nerve. The superior laryngeal nerve
and the pharyngeal branches of the vagus nerve were especially at risk.
Less frequently injured were the glossopharyngeal and spinal accessory
nerves, the sympathetic chain, and the mandibular branch of the facial
nerve. More than one of these nerves was injured in roughly one-third of
these patients. In this same series, 33 percent of patients required
ligation or resection of the ECA. The lCA required reconstruction in 25
percent and was directly repaired in an additional 9 percent. The
carotid arteries were temporarily clamped in 9 percent. Patients in this
series who underwent arterial repair required significantly more
transfused blood (5.67 U versus 1.92 U) and had a higher complication
rate.
Patients with larger tumors tend to
have a higher incidence of cranial nerve and arterial injury. Other
complications resulting from the surgical therapy of these lesions are
infrequent but may include venous graft occlusion, hemorrhage, internal
carotid artery spasm, and respiratory failure secondary to aspiration.
Preoperative embolization, especially for larger tumors, may reduce
these complications
The basic principle behind successful
surgery for carotid body paragangliomas is preoperative preparation and
early intraoperative identification of neural and vascular structures.
This can be achieved by using a wide exposure, intraoperative monitoring
of cerebral blood flow and electroencephalographic activity, peri
adventitial tumor dissection in an inferior to superior direction,
appropriate grafting or shunting of the lCA, appropriate parotid gland mobilization, and meticulous
haemostasis and microtechnique.
The patient is placed supine on the
operating table and general anaesthesia is induced. A nasoendotracheal
tube is used to allow maximal upward displacement of the floor of the
mouth. The operative field that extends from the clavicle to above the
superior extension of the pinna of the ear is then prepared. Routinely,
the ipsilateral lower extremity is also prepared for saphenous vein
harvesting. Although for cosmetic considerations a high horizontal
incision may be used for very small tumors. typically a vertical
incision is used. Tumors that extend into the posterior
fossa should be approached by a separate suboccipital craniectomy.
The initial goal of the operation is
to identify specific neural and vascular structures. The
distal lCA is isolated first. This requires mobilization of the parotid
gland. Therefore. once the skin incision has been made, the superficial
cervical fascia is opened and the posterior border of the parotid gland
is elevated. The temporoparotid fascia between the parotid gland and
the mastoid process is then incised and the main trunk of the facial
nerve is identified. The lower division of the facial nerve and the
marginal mandibular nerve are dissected free and the deep cervical
fascia is divided. The parotid gland is then gently retracted
superiorly. The digastric muscle, stylohyoid muscle and stylomandibular ligament are then divided in turn to expose the distal
lCA. The proximal CCA is then exposed and loose rubber tourniquets are
placed around the lCA, ECA and CCA. Some authorities recommend
obtaining baseline preocclusion and occlusion 131xenon cerebral blood
flow measurements at this point in case rapid occlusion of the lCA is
required later for hemostasis. Next, the neural elements are
identified. The submandibular dissection is continued and the course of
the vagus nerve is identified (it may be incorporated within the tumor
bed). The hypoglossal nerve, which is usually displaced posterosuperiorly, and the spinal accessory nerve are also identified
proximal and distal to the tumor and are tagged.
Tumor dissection begins by outlining
the superficial medial and lateral margins of the tumor. Major arterial
and venous feeding and draining vessels are identified and occluded. A
peri adventitial tissue plane is developed near the bifurcation of the
CCA at the lower end of the tumor. This allows coagulation of numerous vasa vasorum in this area that supply much of the blood supply of the
tumor. Once the tumor has been at least partially devascularized, the
superolateral portion of the tumor is mobilized away from the cranial
nerves and the lCA under magnified vision. Finally, the posteromedial
subadventitial attachment of the tumor is elevated and the superior
laryngeal branch of the vagus nerve is dissected free. Great care must
be taken in this region not to inadvertently enter the carotid artery.
While temporary occlusion of the carotid artery or intravascular
shunting is used routinely by some authors, it is usually not necessary.
Once the tumor is removed, the arterial walls are inspected carefully
and cerebral blood flow may be measured again. The incision is then
closed in anatomic layers, incorporating multiple closed suction
drains.
Surgical Therapy:
Temporal Bone
Paragangliomas
The particular surgical approach used
to resect temporal bone paragangliomas depends on the location and
extent of the tumor. Paragangliomas originating from the promontory of
the middle ear and isolated to the mesotympanum can
be resected by elevating the tympanic membrane and removing the tumor
using microdissection techniques. If the tumor extends into the
hypotympanum or the mastoid, a tympanomastoidectomy is performed and the
tumor resected.
Larger tumors that involve the jugular
bulb or extend medial to the jugular bulb require more extensive
dissection. Fortunately, with recent advances in the techniques of skull
base surgery, extensive temporal bone paragangliomas can be resected
completely by an experienced multidisciplinary team. For example,
Jackson et al. reported on the treatment of 49 patients with skull
base tumors with intracranial extension of which 36 were paragangliomas
originating in the temporal bone. In this series of formidable tumors,
76 percent of patients had gross total tumor resection and most of those with incomplete removal
were operated on early in the series. Now, according to these authors,
tumors that involve the ICA or basilar artery, the foramen magnum, the
cavernous sinus, or the clivus should no longer be considered
unresectable.
Unfortunately, accurate data regarding
the ability of surgery to cure these tumors are not available. Among
those patients in the series referred to above with complete resection
of a temporal bone paraganglioma, there were two recurrences after a
mean follow-up of 5.1 years. One patient with incomplete resection
accounted for another recurrence. Another series reported a single
recurrence among 17 patients with temporal bone paragangliomas, but the
follow-up time was not clearly stated. Still, these tumors usually grow
slowly, and recurrent disease cannot be excluded for many years after
surgical intervention. Therefore, meaningful results about the effects
of aggressive modern surgical techniques on temporal bone paragangliomas
will not be available for another decade or more.
Such aggressive resections in patients
with larger tumors. however, are not without significant risk of
complications (Table-6). For instance, in the series of
Jackson et al., which is representative, 5 of the 49 patients died
within 1 year of surgery. Furthermore, only 24 percent of patients
escaped cranial nerve deficit with 47 percent of patients sustaining
injury to the ninth and tenth cranial nerve complex. No patient in this
series, however, required permanent tracheostomy or gastrostomy tube
alimentation. Enhanced neural preservation can be achieved with smaller
lesions and this underscores the need for
early diagnosis and treatment of these lesions. Irradiation prior to
surgery may also curtail cranial nerve preservation. A number of
approaches to temporal bone paragangliomas have been described. Most of
these are used to excise tumors without intracranial extension or as
the first part of a two-stage operation where an intracranial tumor is
removed through a separate suboccipital craniectomy. More recently, a
number of combined approaches have been developed that allow tumors with
a large intracranial component to be resected by a multidisciplinary
team during a single operation.
TABLE-6 Representative Operative
Complications and Outcome from Resection of Temporal Bone Tumors
Mortality
8%
Tumor recurrence
8%
Wound infection
11%
Cerebrospinal fluid leakage
20%
Meningitis
8%
Required treatments
Vocal cord injection
23%
Tracheostomy
8%
Tarrsorrhaphy
19%
After general anaesthesia is induced,
the patient is generally placed on the operating table in the supine
position. The shoulder is then elevated to a variable degree depending
on the location of the tumor or the preference of the surgeon. A more
lateral position allows excellent exposure of the posterior fossa
component of the tumor but compromises tumor removal from the neck and
skull base. A nasoendotracheal tube is used to allow maximal upward
displacement of the floor of the mouth. The pre- and postauricular areas
and the neck are prepared from the clavicle to above the superior
extension of the pinna of the ear. Routinely, the ipsilateral lower limb
is also prepared for saphenous vein and fascia lata harvesting. The
abdominal area is also prepared as a site for adipose tissue donation.
A postauricular curvilinear incision
is then made. This may be extended in either
direction to improve exposure. As this flap is retracted, the external
auditory canal is transected and closed as a blind sac. The attachment
of the sternocliedomastoid muscle and the contents of the carotid
sheath are then identified. The base of the skull that lies behind and
lateral to the jugular foramen must then be exposed fully. This requires
that the sternocliedomastoid muscle and the underlying splenius and
suboccipital muscles be dissected off the base of the skull. Care must
be taken in this step to avoid injury to the vertebral artery. The
dissection is continued until it merges with one proceeding upward from
the neck that has exposed the internal jugular vein, ICA, ECA and the
nerves of the jugular foramen.
The majority of the patients had
intracranial tumor extension. Smaller tumors are associated with fewer
complications.
Here the surgeon must avoid injury to
the inferior petrosal sinus that may merge with the internal jugular
vein after it exits the skull. Branches from the ECA that are supplying
the tumor, usually the ascending pharyngeal, posterior auricular, and
occipital arteries are occluded. and vascular tapes are secured around
the internal jugular vein, ICA and ECA.
The second stage of the operation
requires the use of a high-speed drill to perform an extensive
mastoidectomy. First, the mastoid process is removed, and then the
sigmoid sinus and the bony labyrinth are skeletonized. If the tumor
extends along the ICA toward the petrous apex, the facial nerve is
uncovered from the geniculate ganglion to the stylomastoid foramen and
transposed anterosuperiorly out of the fallopian canal. A suboccipital
craniotomy or craniectomy is then performed. The portion of the sigmoid
sinus above the tumor is identified. and a ligature is passed through
the dura and around the sinus in this location. A pair of similar
ligatures are also placed around the internal jugular vein (below the
tumor) and the vein is then transected between them. The lateral wall
of the sigmoid sinus may be opened and any tumor invading this wall
resected.
Attention is then turned to the ICA.
It is followed up toward the skull base and into the petrous canal. This
may require transection of the posterior belly of the digastric muscle
and the stylohyoid muscle. Simultaneously, the lateral wall of the bony
eustachian tube is drilled until the isthmus is identified, at which
point the lumen is closed with bone wax and a fascial graft. The tumor
is then mobilized progressively from various directions. As the
superior pole of the tumor is drilled free, one must guard against
opening into the basal turn of the cochlea or damaging the seventh and
eighth cranial nerves. Finally, the jugular vein is lifted out of the
neck and excised along with the lateral wall of the jugular bulb. Here
the medial aspect of the tumor is carefully dissected from the cranial
nerves. As this dissection proceeds, the inferior petrosal sinus with
its multiple openings will be encountered and should be occluded.
Finally, the extradural portion of the tumor is then divided from the
intradural portion and removed.
The intradural portion of the tumor is
then excised. First the dura is opened behind the sigmoid sinus.
Meticulous haemostasis must then be maintained as the tumor
is separated from the parenchyma of the brain. If the tumor encroaches
on the anterior compartment of the jugular foramen. the cranial nerves
in this area may not withstand the manipulation required for complete
tumor removal. Therefore, in this instance, the goal of complete tumor
removal must be weighed against neurological deficit. The same situation
occurs when one encounters tumor that extensively involves the ICA,
basilar artery, clivus, foramen magnum, or cavernous sinus.
Once the intradural component of the
tumor has been removed, the wound is closed. Fascia lata may be used as
a dural graft. The cavity is then obliterated with adipose tissue. A
vascularized temporalis muscle flap can be swung inferiorly and sutured
to the operative margins. The skin is then closed in several anatomic
layers incorporating several closed suction drains. Adjunctive
procedures thought to be necessary such as the insertion of a parenteral feeding catheter, insertion of a lumbar cerebrospinal fluid
drainage catheter, tracheostomy, or insertion of a feeding gastrostomy
tube are then completed.
Glomus jugulare tumors are among the most difficult tumors arising in the base of the skull and considered the most challenging for surgical treatment, since the patients usually come to surgery in advanced state, after failure of adjunctive treatment such as embolization, radiotherapy or previous attempts for partial resection. The neurological state of the patients was usually with involvement of the caudal group of nerves and even with infiltrative destruction of the facial nerve in several cases.
During the period of 1980-2004 I had the experience with 10 cases of what could be considered by Ugo Fisch & Douglas Mattox as class C4De2Di2 tumors. For the academic pools and data concerning these tumors you can follow the references. Here, the main concentration is directed to the personal experience of difficulties during operative and the postoperative period. One case was mentioned in the article: AVOIDANCE OF COSMETIC DEFORMITY IN APPROACHING THE PETROCLIVAL REGION DURING COMBINED TRANSPETROSAL APPROACH.
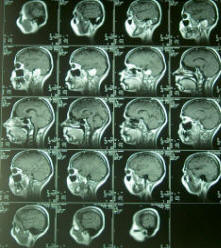
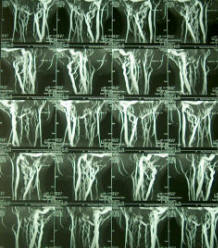
Case Presentation:
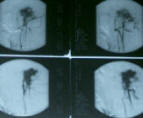
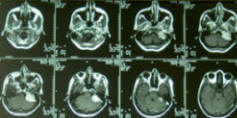
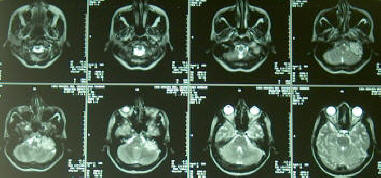
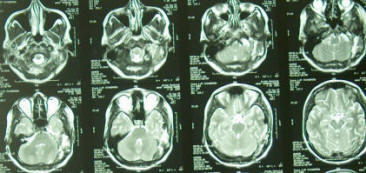
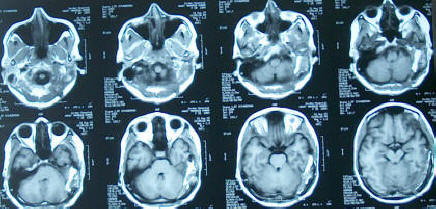
A young married women 27 years age came to the clinic 30-04-2003, complaining of severe headache for more than 3 years duration with hearing loss in the left ear for more than 2 years, ataxia for 11 months, swallowing difficulty for 9 months and complete left facial paralysis of peripheral type for 4 months with right sided hemiparesis and hypalgesia. MRI performed 22-07-2001 showed a mass in the left jugular bulb extending to the sigmoid and transverse sinuses left side. Attempt for embolization caused visual field scatomas . MRI done 12-01-2003 showed enlargement of the tumor four times in volume. The patient on examination, beside the above mentioned complains showed severe atrophy of the left side of the tongue with uvula sagging to the right in gag reflex. It was impossible to perform Romberg test due to inability of the patient to stand. Slight paresis of the left abducens nerve was noted and the voice was dysphonic.
Preoperative angiogram and MRI showing the glomus jugulare tumor shifting the brain stem and totally destroying the left middle and inner ear structures.
The patient was admitted to Al-Shmaisani hospital in Amman - Jordan and operated 17-05-2003. Using the modified trasotic translabyrinthine approach with preservation of the mastoid shell as described
elsewhere, it was possible to track the facial nerve, which seemed to be completely destroyed by the tumor. The inferior margin of the approach was extended to expose the IJV, which was checked for patency. It turned to be completely occluded and after its ligation below the involved mass, it was opened. resection of that part was achieved.
The facial nerve at its emergence from the brainstem was anastomosed using sural nerve to the postfallopian part. To achieve good alignment of the proximal part , 2 hours spent to put three 10 zero nylon stitches. Using artificial tubes , was impossible due to insufficient length of the proximal part. The dura was closed leaving intentionally small defect to the anastomosis, to avoid mechanical pressure and the defect was glued by small piece of muscle. A muscle was harvested from the lower abdomen with fat to fill the spaces under the bone flap , which was reflected back and closed.
The operation took more than 20 hours and the patient required 16 units of blood and 12 units of FFP. Postoperative period was surprisingly unremarkable and she was not in need for tracheostomy, which was highly suspected. NGT feeding was continued for 2 weeks, due to deterioration of the caudal group of nerves , as usual and the left abducens nerve became completely paralyzed after the operation, despite the fact, that it was not touched or violated during surgery.
You can refer here! for more details.
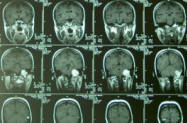
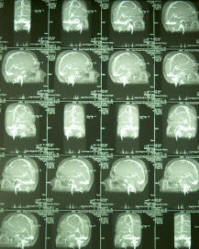
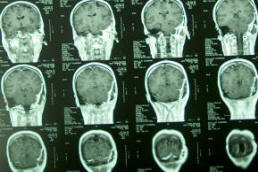
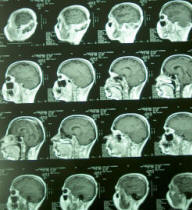
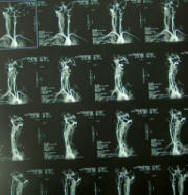
MRI, MRA, MRV of the patient performed 28-07-2003 demonstrating the radical resection of the tumor and bone flap holding the muscle harvested from the quadriceps muscle
The patient was seen several times at ambulatory first with stitch sinus and the left abducens was completely paralyzed. The patient then slowly, but steadily showed marked recovery of her hemiparesis , hypalgesia and the left trapezius became more stronger . The abducens became fully functional after four months. The atrophy of the left side of the tongue regressed and the swallowing and speech dramatically improved. After 9 months the facial nerve start to show dramatic signs of recovery. The patient came 12-12-2004 with almost complete recovery of her facial nerve function.
Discussion:
Conclusions:
References:
Jon H. Robertson, M.D., Jason A. Brodkey, M.D. Glomus Jugulare Tumors. The Practice of Neurosurgery. GeorgeT. Tindall, Paul R. Cooper & Daniel L. Barrow. Volume 1. 67: 1005-1020.
Ugo Fisch & Douglas Mattox: Classification of Glomus Temporale Tumors in Microsurgery of the Skull Base . Thieme 149-153.
The author have made every effort to trace the copyright holders for borrowed material. If inadvertently overlooked any, will be pleased to make the necessary arrangements at the first opportunity.