|
Comments:
1. As seen in the picture the midline incision is
the less traumatic approach to the postganglionic part of the roots.
Dissection to go around the paraspinal muscles is not wise and cause
more trauma to the soft tissues.
2. The integral part of the operation is not to
cause harm to the patient. For that only functionally unimportant
neural grafts must be harvested and they are at maximum 4 nerves
from each leg: the sural, saphenous, anterior cutaneous branch of
the femoral nerve and posterior cutaneous branch of the sciatic
nerve, which is missing in this case due to previous operation for
the bed sore.
3. Using microscopic facility the grafts were
anastamosed using 6 zero nylon. During that the postganglionic
truncks were partially resected to leave the posterior wall of the
epineurium so as to use it as traction to the anastamostic
site. The number of stitches was governed by achieving perfect
alignment of the anastamosis. It was necessary to put between 6 to
10 stitches at each site to regain the goal.
4. Routine closure of the wound and as seen the
grafts are hanging lax and free above the laminaes with luxury
length, to avoid traction in case the patient bend his back.
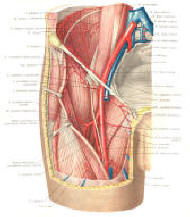
5. From the previous part it became evident, that
only three major branches could be accessible to be used for
grafting for the intended purpose. The posterior cutaneous branch of
the sciatic nerve in this condition was impossible to harvest,
because plastic grafting of the thighs were performed for the bed
sores.
6. This means that such surgery could be applied to
paraplegics below D10 to make the bridges to L1-S1 roots. Of
course, the paraplegics below D9 can have benefit from such surgery,
but with less benefit.
Comments: 1. this is the third
performed operation, and with the increased number of the operations
and with time and end results will be clear. The first performed
operation was in
28-January-2004 which gave partial but excellent results
concerning the anastamosed nerves. He could show the improvement of
some muscles and sensation of some roots, but the operation was not
organized enough to make him able to walk, due to several factors,
among them the negligence of the patient for his situation and
disappearance of the patient mostly due to financial reasons. He
came only once to me 18 months after the surgery and I was
astonished with the good reinnervation of the grafted nerves.
2. The surgical standards are becoming more
standardized and the steps of the operation becoming more precise.
The maximal 8 grafts harvested govern the limitations of the
operation and the number of the lost grafts in the patient also play
a major impact in the decision-making. 3. This
operation can be applied not only to paraplegics, but also to
stationary post-transverse myelitis and other conditions, where the
certain roots for good lost their function. 4. The
fact that the dorsal roots supply relatively small segments of
dermo-myotoms make some skepticism about the final result of the
operation and the presence of 2 stitching points to fill the gap and
the sensory nature of the grafted neural material, all play a
negative theoretical role in the outcome. Time will tell.
|