|
The patient came to the clinic 19-June-2006 complaining of
difficulty in walking, dragging his right lower limb with loss of
sensation below D2 more pronounced in the left lower limb. The
patient started to to complain of this at 6 years age with sudden
onset of paraplegia. The patient was considered as a case of
syringomyelia and shunted twice. The first time it was 2002.
Deterioration took place 2004 and another time was shunted. He
improved for 2 months, but then start to deteriorate with urine
retention.
MRI performed recently, showing a mass extramedullary anterior to
the spinal cord, more to the right at the level of D2-4 resembling
an ependymoma, but it could be an astrocytoma with cystic
degeneration.
On examination: analgesia below D2 with crude sensation preserved
in the right lower limb, which was more weak than the left with the
quadriceps 4/5, knee abduction and adduction 3/5 with inverted foot
and dorsi and planterflexion 3/5 of the left foot. The left foot had
power of the muscles 4/5.
The old incision was refreshed and further drilling to the right
side was performed to attack the spinal cord from the right. The D4
right dentate ligament was released and bisected. The atrophied
right Th4 root was resected to have ample to the latero-anterior
parts of the spinal cord. The anteriorly located cystic component
was opened and evacuated. The violate soft consistency part of the
tumor had no proper cleavage to separated it from the lower pole of
the cyst, which was stuck and diffusely infiltrating the spinal cord
. Biopsy was taken and frozen section confirmed the presence
of low-grade astrocytoma.
Inspection of the spinal cord at the lower edge of the pathology,
showed some firm consistency, than usual, but without mass effect.
The sac was dissected and removed in most parts. It was possible to
see the previously inserted shunt, which was full of adhesions and
has continuity to the spinal cord mass. It was decided not to touch
it. The right Th1-2-3 were seen hanging free with severe
atrophy. The spinal cord was stuck to the dura in the left side and
it was decided not to release it, to minimize the surgical trauma.
Routine closure of the wound.
The patient showed immediate postoperative considerable deterioration
of his neurologic deficit. But sensation of the left foot became
better and sensation of the right foot deteriorated with gross
weakness both lower limbs.
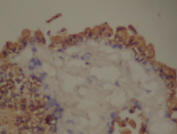
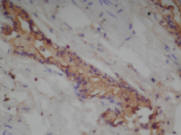
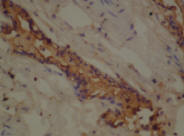
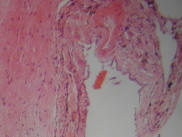
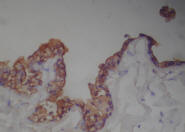
The final histologic verification was that of neurenteric cyst,
which was confirmed by immunohistologic studies.
The patient progressed the fifth postoperative day CSF leak from
the wound. Tension sutures were applied at the ooze point. The next
day CSF leak took place above the previous level and another tension
sutures applied.
The patient during the night round 19-Jly-2006 progressed melena
with diarrhea with hypotension and Hb 8.4 mg/dL. Decadron which was
in tapering stage stopped and nexium with blood and FFP transfusion
were started at the ICU.
Endoscopy of the stomach and the duodenum demonstrated "old
ulcer" in the duodenum and conservative measures were undertaken.
The patient bled three times at 3 days interval and the last one was
the night of 26-July-2006, for what urgent laparatomy was performed
and closure of the ulcer and control heamostasis was performed.
During this time the spinal surgery wound healed properly with no
CSF leak for 2 days.
Comments: 1. It is hard to
tell which tumor in the MRI before the surgery, as in this case.
This tumor was noted in the early MRI , but was not reported and
evacuation of the cyst did not arrest the progression of the
disease. 2. Syringomeylia usually stay intramedullary. The
existence of extramedullary extension of the cyst must hold
suspicion about the nature of the lesion, which proved to be
neurenteric cyst. 3. Despite the fact, that the left 2/3 of
the spinal cord was not exposed to the field of the surgery,
deterioration of the motor function took place at that side. It is
mostly reactionary in the immediate postoperative period. Time will
tel. The patient is covered with dexametasone 16 mg 8h. 4. What is
neurenteric cyst?
In summery: Neurenteric cysts are infrequently reported congenital
abnormalities believed to be derived from an abnormal connection
between the primitive endoderm and ectoderm. Children present more
commonly with cutaneous stigmata of occult spinal dysraphism(OSD)
whereas adults present primarily with pain. Neurological deficit as
a presenting symptom is less common, a finding that reflects the
slow growth of these lesions. In most patients some form of
vertebral anomaly is associated with the cystic lesions, including
Klippel–Feil abnormalities. There is a high incidence of associated
forms of OSD including split cord malformation, lipoma, dermal sinus
tract, and tethered spinal cord. Neurenteric cysts are more common
in the cervical region and in a position ventral to the cord.
These cysts most commonly occur as intradural, extramedullary masses
in the thoracolumbar region, situated dorsal to the spinal cord.
Complete excision of the neurenteric cyst remains the treatment of
choice, as subtotal excision is associated with recurrence. For more
details
click here! 5. The patient is a
young man and he never complain of abdominal problems. The
endoscopic finding of chronic ulcer hold the suspension of the
presence of another anomaly in the duodenum, which could be related
with his primary pathology. |