Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
07-OCTOBER-2018 SARA ABDEL-QADER SHABIB 25
YEARS TUBERCULUM SELLA MENINGIOMA WITH SEVERE COMPRESSION BOTH OPTIC
NERVES AND SUPRA-INTRA AND BILATERAL PARASELLAR EXTENSION AND INVOLVEMENT OF THE LEFT CAVERNOUS SINUS.
Anamnesis
The patient was operated elsewhere for huge
olfactory groove meningioma through subfrontal
approach 6 years ago. At that time the MRI
showed wide dural involvement reaching the left
side of the tuberculum sella with involvement of
the left cavernous sinus. The patient claim that
she lost vision in her left eye for 15 years and
there is paralysis of the left abducens nerve.
The last 3 months, she started to notice rapid
deterioration of the vision of the right eye.
MRI of the brain performed 26-September-2018
showed tuberculum sella meningioma with MRA
showing as be absent left A1 segment. The study
was bad quality.
On examination, the patient needs help to
ambulate due to practical absence of vision. She
has bilateral anosmia after performed first
surgery. Complete blindness of the left eye with
left abducens palsy. Can notice fingers at 10 cm
by rotating the head to certain position. She
has neuralgia like manifestations of the left V2
territory. She cannot look up with her left eye,
denoting the involvement of the left III nerve.
There is scar behind the hair line due to
previous bifrontal approach, which seems that
the anterior bony edge is relatively high.
The patient was sent for investigations and MRI
of the sella and both optic nerves with contrast
showed tuberculum sella meningioma severely
compressing the relatively short optic nerves,
more the left. The pituitary stalk and chiasm
are pushed behind the tumor mass. The left A1
segment is seen and not involved with the tumor.
There is primary optic atrophy of the left optic
fundus with total blindness of the left eye and
seeing the fingers with certain position at 10
cm distance and profound scatoma right eye with
small field of vision at the temporal upper
half.
The old skin incision was
refreshed and reflected to the face. The old bony
flap was reflected to the right ear. It is defective
and not suitable to approach the chiasmal region,
for what another bone window was created to be flush
with anterior fossa. The dura was opened parallel to
the anterior lower edge of the bone defect. Sharp
dissection of the anterior fossa to reach the
chiasmal region. The tumor was seen between both
optic nerves. The chiasma prefixa was the type of
the chiasm. Drilling of the tuberculum sella to
remove the bony part of the tumor and decrease the
vascular supply of the meningioma. Piece meal
resection of the tumor until the right optic nerve
became free of tumor compression. Further
intrasellar resection of the meningioma until the
pituitary stalk and pituitary gland were noticed
behind the tumor. There is left anterior clinoid
tumor compressing the left ICA and left optic nerve.
It was resected. The intrasellar part of the tumor
is stuck and adherent to the left optic nerve. Sharp
dissection and separation of tumor from the
compressed left optic nerve. Radical resection of
the tumor and no residual f the tumor to compress
the left optic nerve. The pituitary gland and stalk
were seen behind and the chiasm was hanging free.
Both supraclinoid ICAs are free and all the time
irrigation with Papaverine was applied to prevent
possible arterial spasm. The tumor was separated
totally from the left cavernous sinus. Strict
hemostasis with water-tight closure of the dura.
Both bone flaps were sutured together and fixed in
place, Routine water-tight closure of the wound
with ready Vac under the skin.
Smooth postoperative recovery. She was sent to the
ICU for 24 hours observation. The patient is
claiming that the vision in the right eye improved
and she can feel light in the left eye.
Comments
The patients is losing the vision of the
right eye in addition to the totally lost vision of the left
15 years ago. Surgery is a must to rescue the pending
bilateral blindness.
Follow Up
The at the same day after surgery,
noticed slight improvement both optic nerves function, but
the next day she lost vision in both. The day after she
regained slight improvement of the vision of the right eye,
but less than before surgery.
The patient was admitted 30-October-2018
with nausea and vomiting and MRI of the brain (Fig-13 and
14) ruled out any intracranial problems. Lab investigations
were normal and she was seen by gastroenterologist and
endoscopy confirmed presence of hiatal hernia and ulcerative
gastritis. She told us that after the first performed
surgery, the same episode happened and for 3 months suffered
from this situation. We stopped all medications and kept her
in nexium twice daily and zofran 8 mg three times a day.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Head mounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
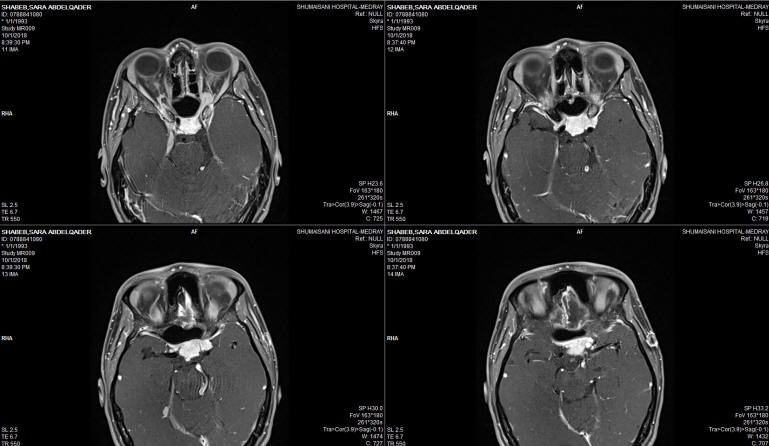
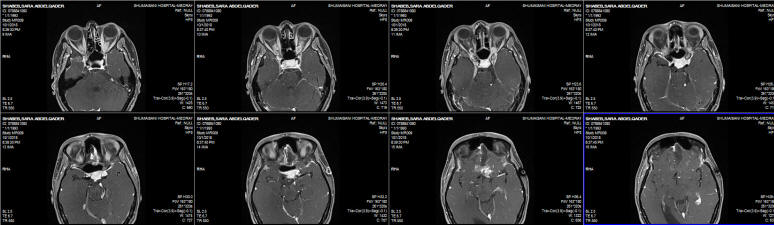
Fig-1: Axial view with contrast.
Fig-2: The data as above with more cuts.
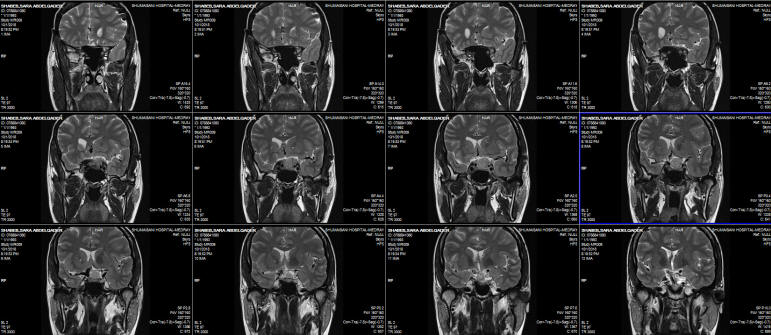
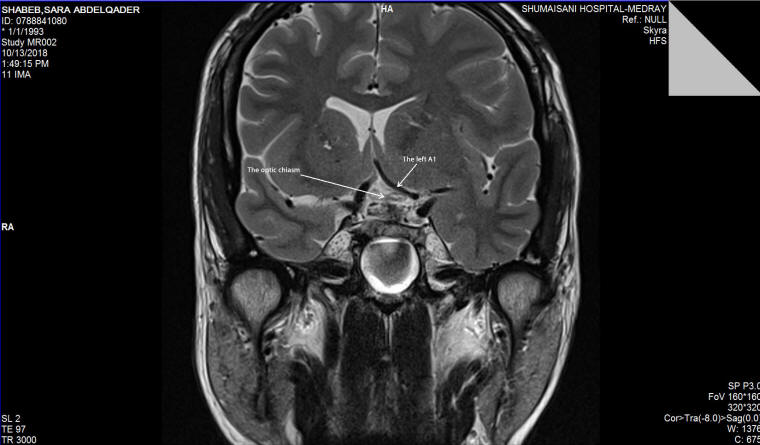
Fig:-3 Frontal view without contrast showing the pituitary stalk and
chiasm pushed behind the tumor and the presence of the left A1
segment.
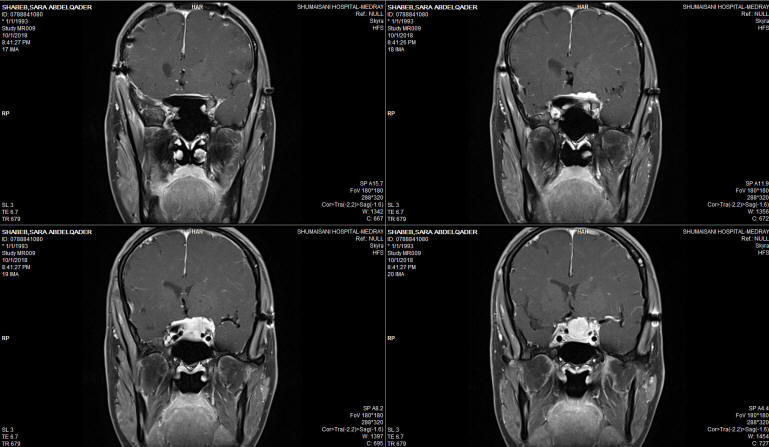
Fig:-4: Frontal view with contrast showing with wide extent of the
tumor carpet.
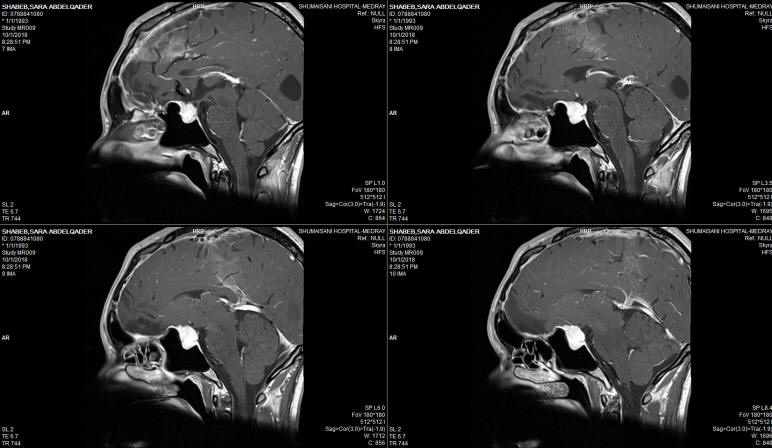
Fig-5: Saggital view.
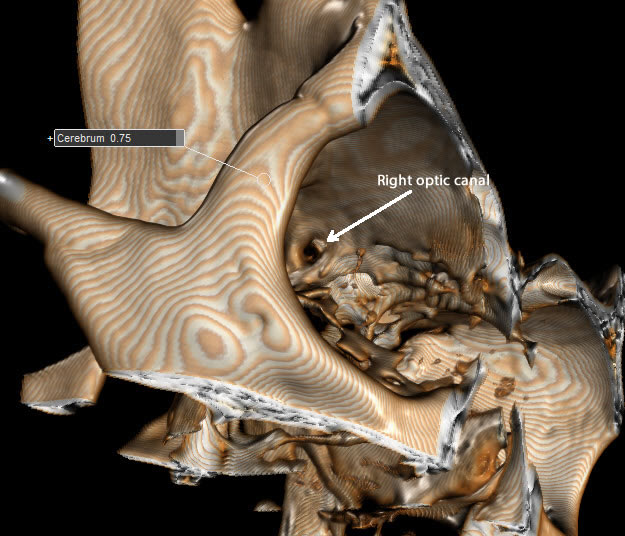
Fig-6: The right optic nerve after reconstructing the CT-scan using
ORS Visual.
Fig-7: The optic chiasm and right ICA after total removal of the
tumors. Notice that the tuberculum sella was drilled off to reach
the intrasellar area due to chiasma prefixa variant.
Fig-8: MRI performed 6th postoperative day showing the free chiasma
prefixa.
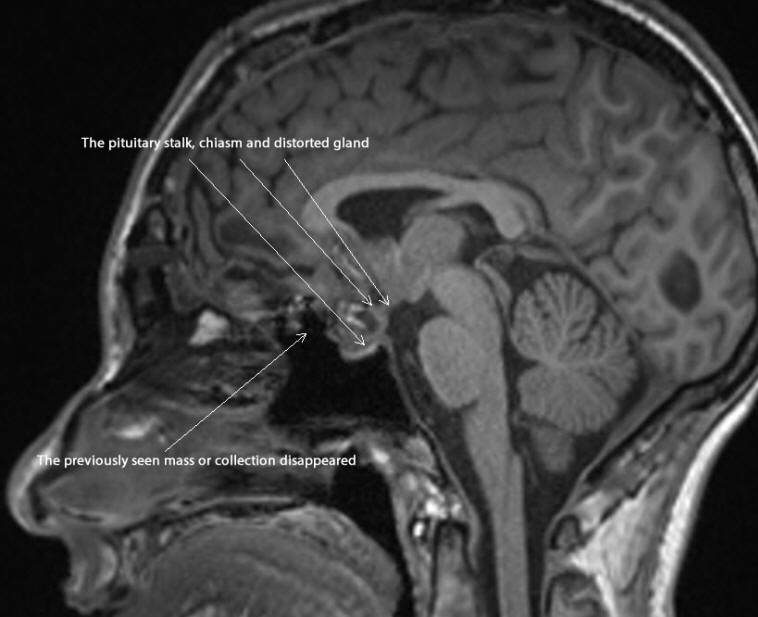
Fig-9: MRI Saggital view performed the 6th postoperative day showing
the swollen pituitary gland and stalk.
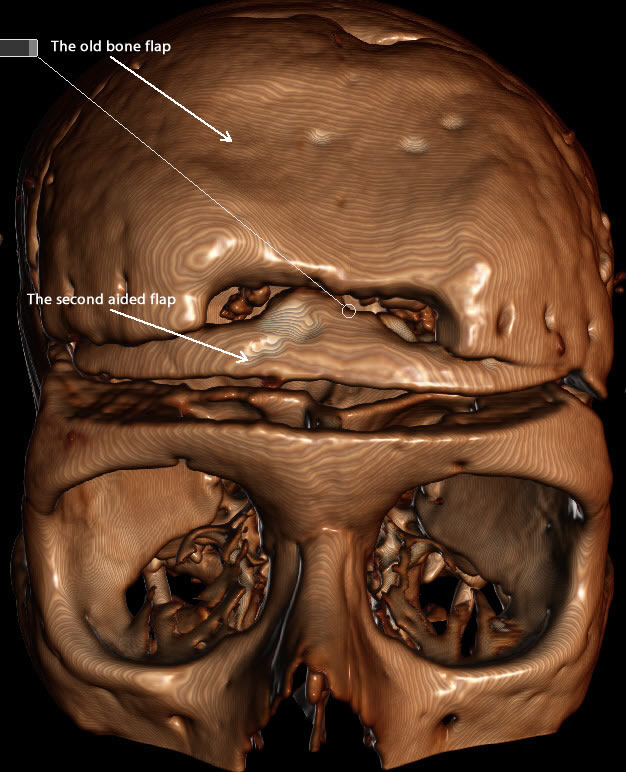
Fig-10: The new created bone flap to obtain proper approach to the
chiasmal region.
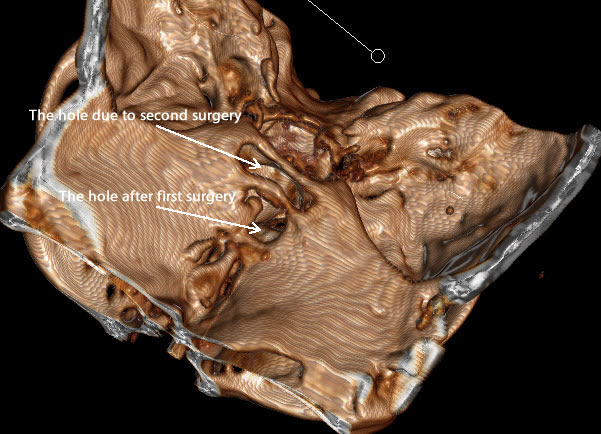
Fig-11: The bone defect after first surgery and the second due to
drilling of the tuberculum sella to reach the sellar area due to
chiasma prefixa.
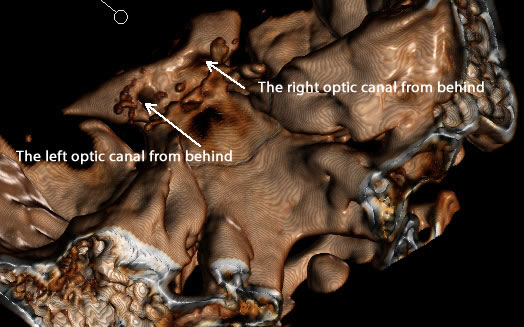
Fig-12: It is now possible to see both optic nerves from behind
after the performed surgery.
Fig-13: MRI performed 31-October-2018 showing some reduction of the
distorted anatomy and disappearance of collection under the previous
operation, ruling out progression of CSF leak.
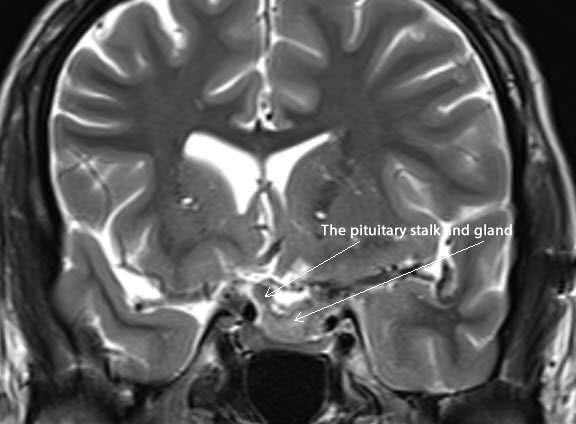
Fig-14: same investigation with frontal T2W protocol.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .