Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
28-MARCH-2022 ZIAD ADEL YAMAK 40 YEARS LEFT
TRIGEMINAL NEURALGIA.
Anamnesis
The patient came to the clinic
20-July-2016 complaining of left trigeminal
neuralgia for 1 year. MRI done 21-September-2015
and 24-January-2016 showing a possible loop of the SCA
compressing the left trigeminal nerve. There was
suspicion of meningioma with hyperostosis which
was denied. The
patient is neurologically free and all
medications failed to improve his condition,
instead causing sleepiness and drowsiness.
On examination, the patient is neurologically
free. except for the left trigeminal neuralgia.
The patient came several times and the last time
came 17-March-2022, urging for surgery. He is in
Tegretol 200 CR three times a day. Higher doses
causing drowsiness.
In lateral position, with the
left mastoid at upper position and Mayfield
clamps fixed to the head. Epidural kit with
catheter 20F was inserted intradurally and 40 cc
CSF regained and the catheter was kept in place.
Using the navigation, the junction between the
transverse sinus and the left sigmoid was
identified. Vertical retromastoid incision was
done. A small bur hole was created at the
junction. Using the footed attachment of Midas
Rex a small craniotomy was done. During that
massive bleeding took place. The bone was
removed and the source of bleeding was an
abnormal emissary vein projecting from the
transverse sinus. Until closing the dural defect
of the sinus with 4 zero nylon, the patient lost
1.5 liter of blood. The anesthesia team was
warned that something wrong with his venous
return, because in the usual circumstances it is
usually easy to manage this situation without
such loss of blood. The dura was opened inferior
to the left transverse sinus and extended down
parallel to the sigmoid sinus. The cerebellum is
tight and further elevation of the head was
achieved and more CSF was drained. The
cerebellum was stuck with tentorium and sharp
separation was needed to achieve the goal with
difficulty. The family were interrogated if the
patient suffer previous head injury. The mother
telling that when he was 8 months age, he
suffered severe head injury with fracture of the
base of the skull. Taking this fact in
consideration, the patient was put in setting
position with the left mastoid up. The
navigation was reapplied another time. After
that the cerebellar structures became lax and
the work with the scars was more easy. There was
no superior petrosal vein and dissection was
followed until the tip of the left petrous bone.
There is hypertrophic callus formation
compressing the left trigeminal nerve. Drilling
of the callus formation and widening the edges
around the trigeminal nerve was achieved with
the smallest size of Smith Kerrison. Inspection
was carried out from the trochlear nerve down to
the facial and vestibulo-cochliar nerves. There
is no compressing arteries or veins. Using motor
stimulation was negative. Check in the muscles
with 10 Volts was negative. The anesthesia was
told to to stop the muscle relaxants and were
asked how much time it will take to wear the
effect of muscle relaxants. They told me it will
take 20 min. During that bipolar pulsed mode RF
with 42 Celsius, 240 sec, 2 Hz and 20 msec
duration to the left trigeminal nerve was
achieved using 2 bended catheters 10 mm exposed
length. After wearing of the muscle relaxant,
the facial nerve responded well to 0.7 Volta and
the trigeminal nerve to 1.5 Volts. Strict
hemostasis and the dura was closed with lyodura.
The bone was removed in place and the wound was
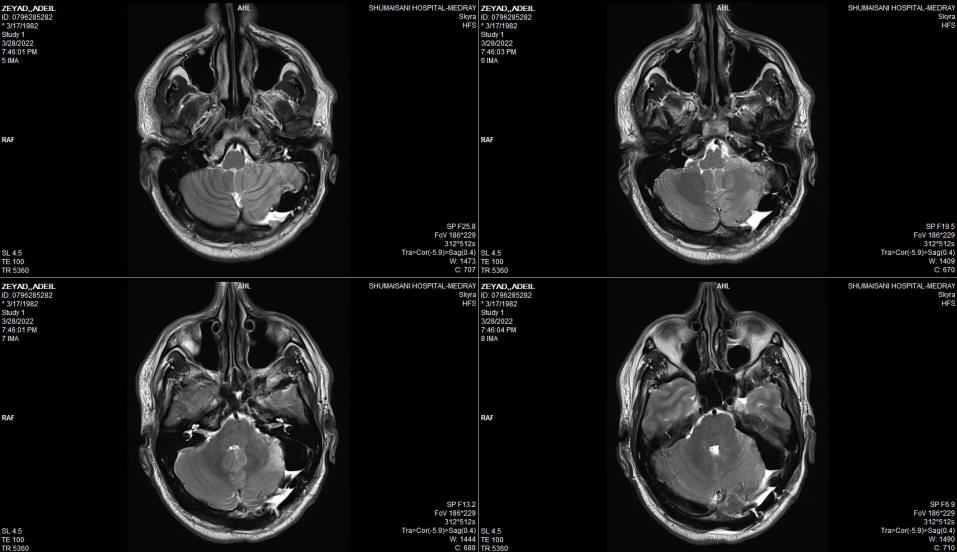
closed. Before extubating him, check MRI was
done showing an acceptable picture with some air
in the upper field of operated area and small
amount of blood at the bottom with edema of the
lateral part of the the left cerebellum. The
patient was extubated smoothly and the patient
was sent to the ICU. The operation took 12 hours
duration.
MultiGen
FOLLOW UP
The patient 29-March-2002 is suffering from
paresis of the left facial nerve, but closing
the left eye. Hearing is preserved and has
numbness of the left side of the face. The gag
reflex is preserved and protruding the tongue
normal with normal gag reflex. There is
nystagmus to both sides and complaining of
double vision, but the left abducens is
functioning properly. Refusing to swallow
liquids, despite the fact, that he has normal
swallowing.
The next day in the ICU 30-March-2022 with
difficulty, he was put in setting position
several times and he is afraid to swallow
liquids. The cough
reflex was exaggerated and it was explained to
him, that the liquids he is swallowing are not
related to the sputum and he was encouraged to
have more fluids. He was encouraged to put him
in setting position several times to decrease
the vertigo.
In 31-March-2022 the patient was encouraged to
have a walk near the bed several times and and
the Foley's catheter was removed and he was
encouraged to have more walks and to urinate in
the bath room and to have more amount of fluid
diet. Check for hypothyroidism was negative.
The patient was seen by ENT specialist
5-March-2022 and barium swallow was performed
showing tiny residual slipping to the
epiglottis, due to edema and making him afraid
to feed him by mouth, for what naso-gastric tube
was inserted 6-March-2022 and he was discharged
the following day to be kept with the NGT for 2
weeks. Upon discharge the patient is pain free
and walking with mild support with continued
improvement of his left sided facial paresis.
The patient then came 28-April-2022 with PEG
inserted 3 days ago for feeding and still
complaining of swallowing difficulty, but can
swallow soft food such as yoghurt. The left
facial nerve regained considerable improvement,
but the patient noticed loss of hearing left
side the last week. The left trigeminal nerve
still having hypoesthesia for tactile, thermal,
and pin-brick sensation. Still having horizontal
nystagmus, but the double vision disappeared.
Still need support when walking due to ataxia.
Still having numbness of left V3, but no more
neuralgia.
The patient then came 26-June-2002 complaining
of double vision, complete hearing loss left
side, but he walk without aid with almost
complete recover of the left facial nerve. Still
complaining of swallowing difficulty, but he
mention that the assort of the eating food is
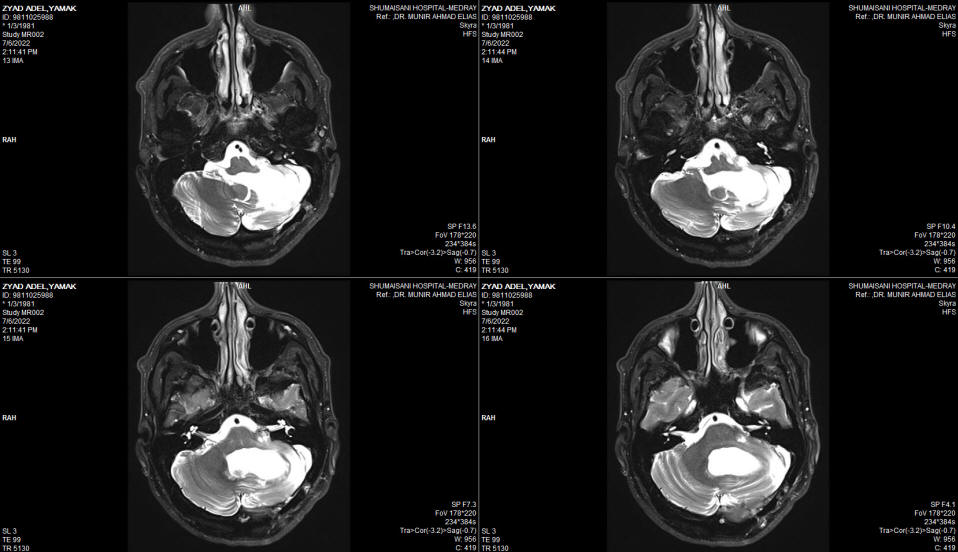
widening, but still using PEG. MRI of the
brain done 06-July-2022 showing massive malacia
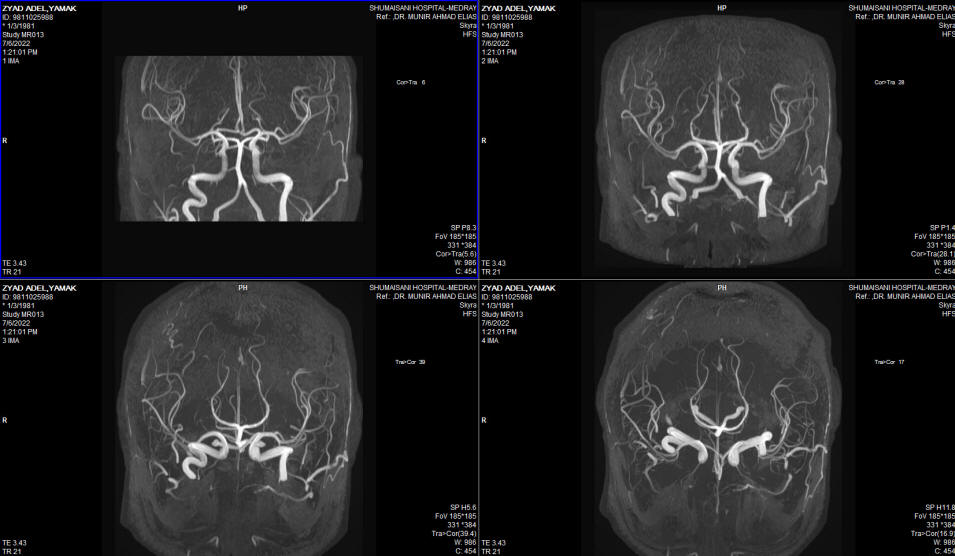
of the left cerebellar hemisphere. The brain
stem and the posterior circulation are intact.
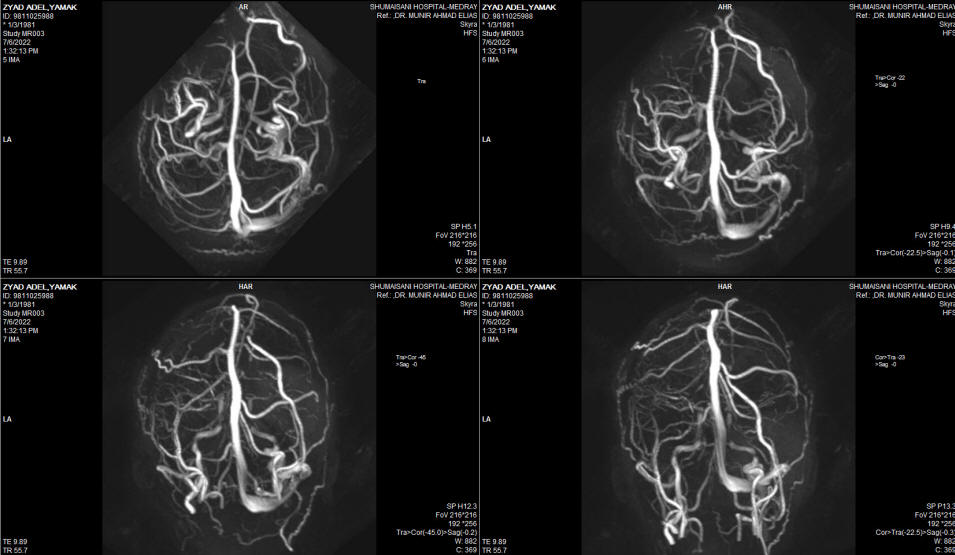
The MRV showing absent left transverse sinus ,
which could be a variant. The left trigeminal
nerve is not compressed and the canal is wide.
Comments
The bony compression with such long time
after trauma can trigger trigeminal neuralgia even after 39
years.
This is the 235th case using the BPRF mode
with MultiGen. This procedure regained routine acceptance.
It became a usual part of the spine and peripheral nerves
surgery. Click here for
reference.
It still unclear to evaluate the
differences of pre and post application motor responses. The
only sure thing that it tells that the electrodes did not
migrate during the procedure and the nerve is functioning
properly. Here it was impossible to evaluate pre and post
application due to muscle relaxant application.
With accumulation of data, it became
clear that the irritated nerve with aberrant currents
running in the C fibers up, not only causing no change or elevation of
the required voltage to achieve motor response, but they could cause the preoperative
weakness. Ablation of such currents results in facilitation
of the motor response and improvement of function with
disappearance of pain.
It is unclear why the roots have several
motor response with different patients, despite the fact
that the neurological status is the same and the anesthesia
protocol also the same.
It could be that the nerve is recovering
minute by minute after decompression and this can explain
why the motor conductivity is improving after the BPRF
application, which require 4 minute session in most cases.
After the 172d case, the elevation of
motor stimulation above 5 V was abandoned to avoid delayed
dural tear with subsequent CSF leak, which take place at the
contact at the lower electrode shaft with the dura below the
level of the axilla.
BPRF to my knowledge is the first case
was included in the treatment of the trigeminal neuralgia
after removing the bony compression. Instead of rhizotomy
or thermal radiofrequency which will trigger the de la Rosa pain, BPRF will ameliorate
the pain, which is the main aim of the surgery.
During the available records since the
last 20 years, 48 surgeries were performed for trigeminal
neuralgia, different scenarios were seen, some finished with
MVD, coagulating the abnormal veins and this is the first
case was post-traumatic with callus formation with bony
compression of the trigeminal nerve.
Repositioning of the patient during
surgery from the lateral to setting position must be
performed with great attention to the endotracheal tube, to
avoid mechanical injury to the larynx, as it took place in
this case.
During surgery, the brain stem was
slightly more solid than usual and the pia matter
surrounding it was thick. Despite all efforts to apply
minimal traction, it could be that all the area reacted more
than usual.
In retrospective analysis, it seems that
the entire left hemisphere was receiving blood supply
through tiny scattered feeders from the inferior surface of
the tentorium. That is the only explanation to such result
of severe malacia and atrophy of the left cerebellar
hemisphere, due to attempt to dissect the stuck hemisphere
to the tentorium to reach the target of action.
The lesson from this case, that it will
be very difficult to anticipate this situation. If
anticipated then direct drilling to reach the area through
the petrous bone from the left side, trying during that to
avoid dissection of the cerebellar hemisphere off the
tentorium. Since this case is very rare it was described in
detail to give a message to the experts in this field, that
this can have place.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Head mounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
LooksCam II Xenosys in the run starting from 14-March-2021 with
SheerVision TTL x4 magnification.
Fig:-1
Intraoperative MRI showing air in the manipulated region and clot
beneath the empty cavity.
Fig:-2
The location of the glossopharyngeal nerve and nuclei are far from
the operative activity.
Fig:-3 Severe malacia and atrophy of the left cerebellar hemisphere
with preserved brainstem.
Fig:-4 MRA of the brain with excellent posterior circulation.
Fig:-5 MRV showing absence of left transverse sinus which could be a
normal variant.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .