|
The patient came
to the clinic 10-October-2006 complaining of right Bell's palsy for
6 days, decreased hearing right ear since childhood. He started to
complain of headache and ataxia for 1 year, disturbed memory
and dyslexia for 3 months. He is a known hypertensive for 12 years.
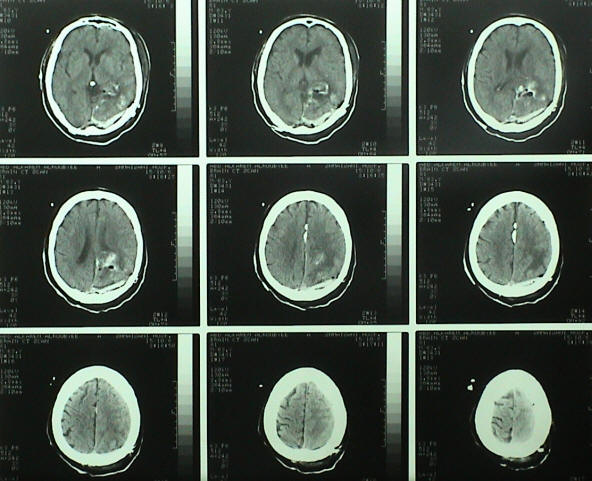
CT-scan done 4-October-2006 showed left occipital meningioma and
suspected right CPA lesion. On examination: the patient has Bell's
palsy, not related to the mass, otherwise the patient was
neurologically free, except for the above mentioned.
MRI of the brain and MRV were performed and showed a giant
meningioma having matrix in the tentorium and falx cerebri posterior
third and invading the posterior horn of the left lateral
ventricle.
The patient in concord position with the face slightly rotated to
the left, a bone flap was performed so as to expose most of the left
occipital lobe and the torcula Herophili and left transverse sinus.
U-shaped dural incision was done parallel to the transverse sinus ,
up to the far point of the superior sagittal sinus and reflected to
the right.
Despite several method to decrees the swelling of the bulged
brain, it was impossible to attack the lesion interhemispherically
and attempts to go supratentorially was difficult without causing
harm to neural tissues. It was decided to attack the lesion
transcortically through 2 cm incision.
The tumor was rubbery and violet in color and very vascular with
multi feeders. Most of the tumor was so rubbery, that it was
difficult to cut it with scissors and No 11 blade. Piece-meal
removal was performed and the matrix of the tumor to the falx
cerebri was bisected and coagulated. The intraventricular part
had it's own feeders and draining veins, which were coagulated and
bisected. The matrix of the tentorium and the tentorial edge was
also coagulated and cleaned meticulously. The last small piece which
was stuck to the junction of the falcino-tentorial junction was
sharply bisected and a 7 mm draining vein was identified, which was
draining to the left deep cerebral vein, was removed after
coagulating this vein and bisection. Radical removal of the tumor
was achieved and the brain regained relaxed appearance and
after that, it was possible to explore the intrhemispheric region
and the supratentorial region. The rectus vein was clean of the
tumor and the tentorial edge was was free with intact arachnoid and
the vein of Labbe was running free.
Routine water-tight closure and smooth postoperative recovery.
The patient blood group was B+ and he received 3 units of blood and
6 units of FFP. The operation took 14 hours.
The next day the patient was doing well and no neurological
deficit escalated. He spoke with all medical personnel and ate and
walked. He was an inelegant one and repeated poems in Arabic. After
30 min of second ambulation, got sudden onset of cardiac arrest,
which did not respond to resuscitation during 90 min with
asystole remained during this time, and his clinical death was fixed
at 2.00 pm. The cause of death was acute massive thrombotic embolism.
For more details about this topic,
click
here!
Comments:
1. Setting position was not adequate for this operation,
because the occipital lobe will be damaged by gravity during work.
2. Concord position is the best option, but the area must be
above the level of the heart to prevent venous congestion, and this
make the position of surgeon very bad and as in this case the
surgeon needs resuscitation in case of more than 12 hour work such
in this case.
3. It is hard to tell which type of meningioma is this one, since it
had matrix in the falx and tentorium and the left lateral ventricle.
When the meningioma reach giant dimensions, it regain a matrix
where it stuck to the dural sleeves and regain pathologic feeders
and draining vein when it invade the ventricle.
3. This operation was the most difficult in my life, since it
include all the factors, making its resection difficult ( rubbery
consistency, highly vascular, multilobulated, has multiple matrices
and stuck to major vessels and veins and important sinuses.
Patience, time, clean surgery, microscopic facility, sharp
dissection and the ability to choose the appropriate exposure
are the key to achieve success in performing such surgery.
4. Old age and hypertension are risk factors for mortality, even for
minor surgeries and this factor increases with major surgeries.
5. Prevention of PE in such highly vascular intracranial operation
remains a dilemma, which needs solution, since anticoagulants are
forbidden during this scenario and despite the fact, that early
mobilization of the patient was taken into consideration with this
patient to prevent such event.
6. The patient progressed the fatal events within seconds and
asystole persisted for 90 min despite the various methods of
resuscitation. Nothing can be done more in this situation at the
present time and only the future can give the answer for the best
practice how to resolve such an event. |