Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
27-NOVEMBER-2016 RAMI SALAH AL-NAJDAWI 30 YEARS
RIGHT BRACHIAL PLEXUS NEURITIS WITH AGONIZING PAIN.
Anamnesis
The patient came to the clinic 26-October-2016
complaining of weak right upper limb for 30 days
with agonizing pain of the right upper limb and
discoloration of the right side of the tongue
and cramps of the left little toe. MRI performed
16-October-2016 was normal with EMG done
24-October-2016 confirming plexopathy.
On examination, the patient has intolerable pain
of the right upper limb neuralgia like, that he
is protecting her from any external stimulation.
The right biceps muscle is 2/5, flexion right
hand 2/5, extension 0-1/5, right triceps 2/5,
There is hypalgesia of the right median and
ulnar nerve distribution. here is no neck pain
upon moving it. DTR D=S, no pathologic reflexes.
There is pain upon palpating the right axillary
artery. No frozen shoulder nor TOS. There is no
myelopathic syndrome.
The patient was sent for neuro-radiologic
evaluation and MRI of the right plexus and right
shoulder were performed
30-October-2016 showing plexitis of the right
brachial plexus at the level of the axillary
fossa. All available lab investigations were
normal.
With the patient awaken, with
the right upper limb extended to expose the
right axillary fossa, 4 catheters were inserted
n both sides of the right axillary artery. Bipolar motor stimulation of
right brachial plexus was achieved with 1.2 V. A
bipolar pulsed mode
RF with 42 Celsius, 240 sec, 2 Hz and 240 msec
duration to this segment was achieved using
2 bended catheters 10 mm exposed length. Further
motor stimulation done to the same points and the
response was 1.1 V with more brisk
response. The same procedure was repeated 3 cm
above the mentioned level lateral to the
axillary artery to ensure more proximal
branches. Bipolar motor stimulation of right
brachial plexus was achieved with 1.2 V. A
bipolar pulsed mode
RF with 42 Celsius, 240 sec, 2 Hz and 240 msec
duration to this segment was achieved using
2 bended catheters 10 mm exposed length. Further
motor stimulation done to the same points and the
response was 1.1 V with more brisk
response. Bipolar motor stimulation of right
median nerve was achieved with 1.7 V. A
bipolar pulsed mode
RF with 42 Celsius, 240 sec, 2 Hz and 240 msec
duration to this segment was achieved using
2 bended catheters 10 mm exposed length. Further
motor stimulation done to the same points and the
response was 0.7 V with more brisk
response. Bipolar motor stimulation of the right
ulnar nerve above the cubital tunnel was achieved with 1.5 V. A
bipolar pulsed mode
RF with 42 Celsius, 240 sec, 2 Hz and 240 msec
duration to this segment was achieved using
2 bended catheters 10 mm exposed length. Further
motor stimulation done to the same points and the
response was 1.4 V with more brisk
response. Bipolar motor stimulation of right
radial nerve from behind was achieved with 0.5 V. A
bipolar pulsed mode
RF with 42 Celsius, 240 sec, 2 Hz and 240 msec
duration to this segment was achieved using
2 bended catheters 10 mm exposed length. Further
motor stimulation done to the same points and the
response was 0.7 V with more brisk
response. This procedure was dictated by the
patient feedback of his pain and it was
continued until he became mostly pain free and
the range of motion improved and the strength of
the muscles dramatically improved.
He was sent to the ward for
discharge.
MultiGen
Comments
The patient has agonizing pain due to
plexitis and all conservative measures to ease his pain
failed.
This is the 94th case using the BPRF mode
with MultiGen. This procedure regained routine acceptance.
It
became
a usual part of the spine surgery.
Click here for
reference.
It is the first case using this procedure
in awake patient confirming that the procedure is effective
and yielding good results without using Marcain or
Depomedrol. Time will tell the length of the effect of this
procedure.
It still unclear to evaluate the
differences of pre and post application motor responses. The
only sure thing that it tell that the electrodes did not
migrate during the procedure and the nerve is functioning
properly. Here there was no change of the threshold of
stimulation power of motor stimulation after the BPRF in one
root and improvement of the other.
With accumulation of data, it became
clear that the irritated nerve with aberrant currents
running in the C fibers up, not only causing no change or elevation of
the required voltage to achieve motor response, but they could cause the preoperative
weakness. Ablation of such currents results in facilitation
of the motor response and improvement of function with
disappearance of pain.
To my knowledge, it is the first case in
human practice, that using such technique in brachial plexus
neuralgia after neuritis giving an excellent result making
the patient and the neurosurgeon happy.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed back about the localization.
Inomed MER system
Leica HM500
The World's first and the only Headmounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014
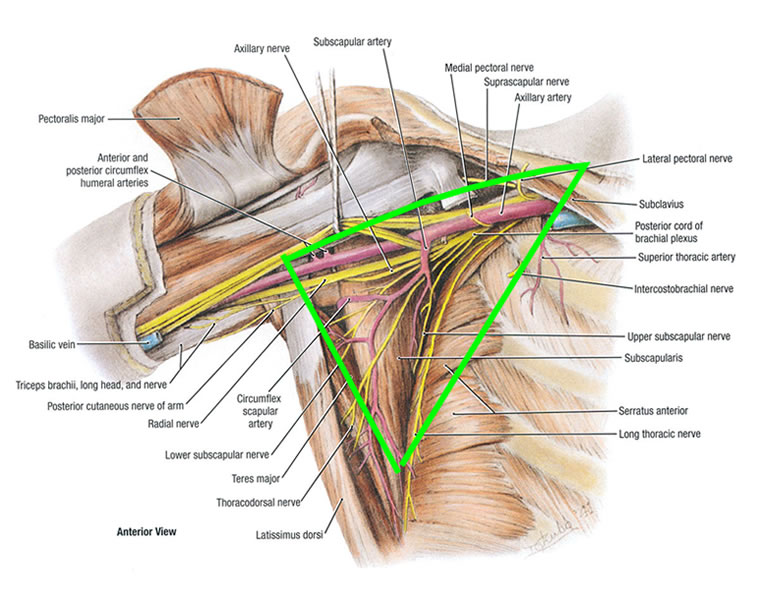
Axillary fossa anatomy showing the relation of the brachial plexus
and its relation to the axillary artery.
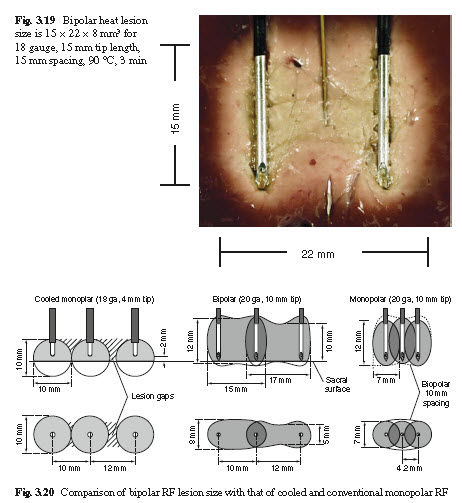
Schematic drawing showing the effective areas of the fields in
bipolar mode of BPRF.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .