Most of the site will reflect the ongoing surgical activity of Prof. Munir Elias MD., PhD. with brief slides and weekly activity. For reference to the academic and theoretical part, you are welcome to visit
neurosurgery.tv
Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
02-JUNE-2012 MUHAMED MAHMOUD MUHAMED SAAYFAN 10 YEARS
LEFT CAROTID BODY TUMOUR TYPE III WITH TEMPORAL BONE DESTRUCTION-GLOMUS JUGULARE
TUMOR.
Anamnesis
The
patient
was
admitted to Shmaisani hospital from Palestine
with complains of left ear pain for more than
one month with hearing loss in the left ear and
Horner syndrome left side and strider and
swallowing difficulty.
On
examination, the patient was alert cooperative,
walking normally with stable Romberg stance with
slight weakness of the left upper limb with no
sensory deficit. He has miosis of the left eye
with enophthalm and ptosis of the left eye and
slight congestion of the left eye (Horner sign).
The vision is not affected nor the oculomotor
nerves. The hearing of the left ear was severely
impaired. There is slight weak muscles of the
left facial nerve. The gag reflex is impaired
from the left and the uvula is sagging from the
left side. The left side of the tongue is
atrophied and shift to the left when protruding
it anterior. The patient is suffering from
swallowing difficulty and has hiccup. The
condition is progressing every day and the
condition is deteriorating. There is hard mass
elevating the lobule of the left ear and
extending down to the bifurcation of the common
carotid artery.
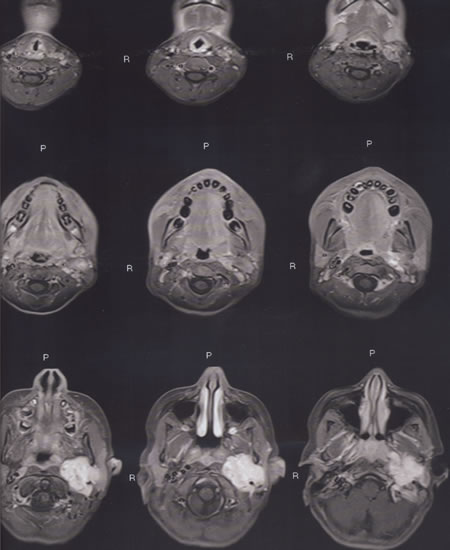
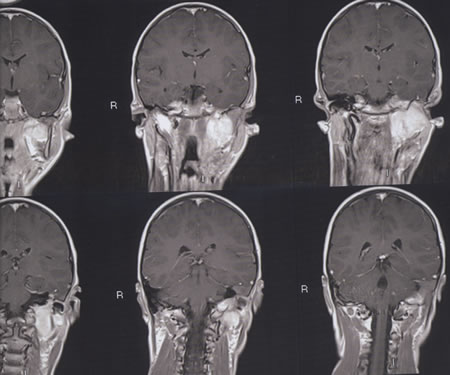
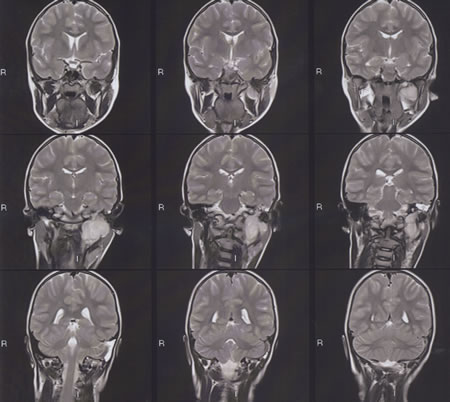
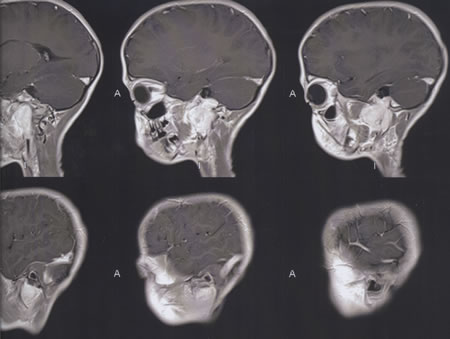
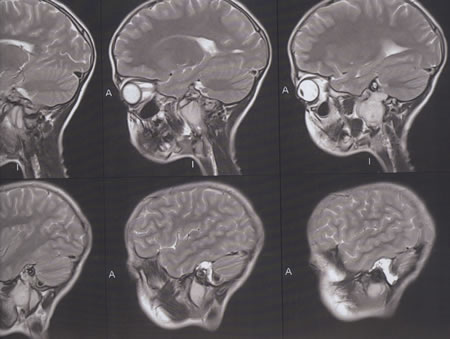
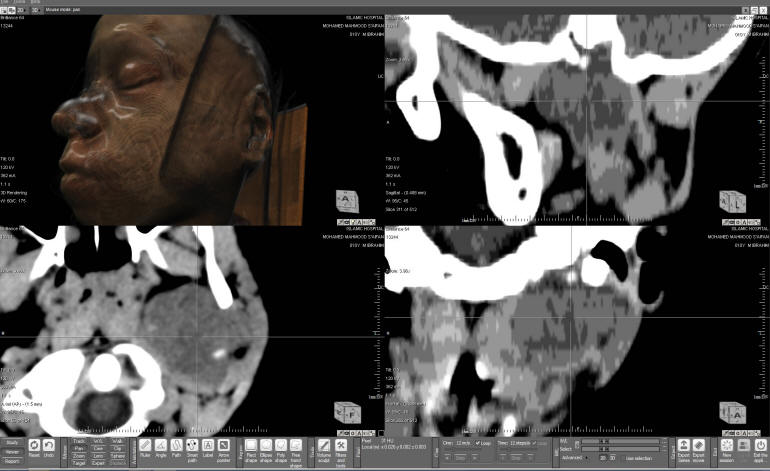
The
patient was sent for investigations and MRI
performed 31-May-2012 showing huge mass
occupying the left temporal region, involving
the middle part of the petrous bone, extending
into the middle ear and to the jugular fossa,
medially to the left parapharyngeal space and
laterally to the parotid area and subareolar
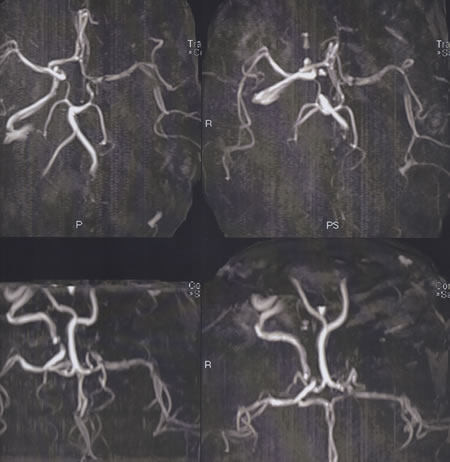
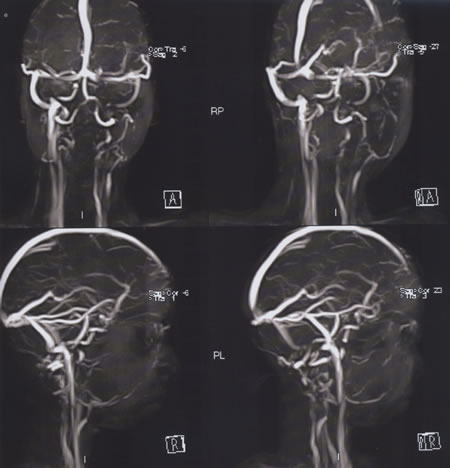
space. MRA showed no flow signal of the left ICA
in the neck and brain. Multiple vascular
branches are seen supplying the mass from the
left ECA. The extracranial MRV showed no flow
signal from the left jugular vein and the
sigmoid, which could be explained by low flow.
The
patient was given Dexamed before surgery, after
what the hearing became normal and the mass
decrease in size.
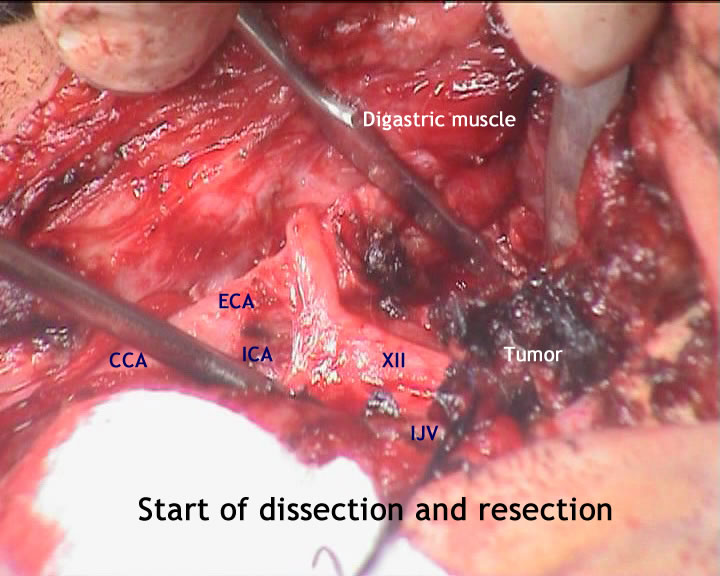
Using Inomed ISIS 32 channel,
INAV Medtronic navigation, and facility for
angiography, the patient was put in prone
position with head rotated maximally to the
right with fixation of the head with Mayfield
fixator, incision anterior to the left
sternocliedomastoid muscle was done to expose
the common carotid, ICA, ECA and the mastoid
tip. The hypoglossal and the glossopharyngeal
nerves were exposed and preserved. The tumor was
hard in consistency and filling the left jugular
vein. Venography of the jugular vein was
performed to see if it is patent and showing any
flow tot eh sigmoid or inferior petrosal vein.
It was negative and only bush of contrast was
seen at the most superior part of the tumor.
Stepwise dissection of the tumor was performed
from the most distal up to the base of the
skull. The jugular vein was ligated by silk. The
occipital, ascending pharyngeal and the
maxillary arteries were the main feeders of the
mass. They were followed and coagulation or
ligation was performed to decrease the bleeding
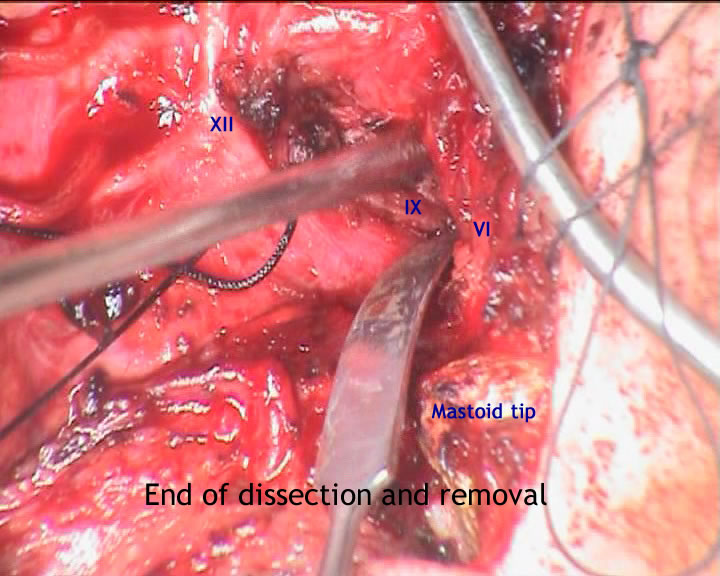
and facilitated the tumor removal. The involved
tumorous jugular vein was followed until it was
reaching the jugular foramen. The anterior parts
of the tumor were removed by piece-meal fashion,
until the dura of the middle fossa was noted.
During this part, the distorted posteriorly
facial nerve was seen and preserved. It was
possible to find this because of Inomed
technology. Subtotal resection of the tumor was
achieved leaving intentionally a part in the
sigmoid sinus to avoid catastrophic sequel. A
big piece of surgicele was applied over the
remaining part of the tumor. There was minimal
blood loss and the patient did not require blood
transfusion.
Routine
closure of the wound. Smooth postoperative
recovery. Horner sign immediately disappeared
and no cranial nerve deterioration was noted.
Please! wait for 3-5 min till the
video start to load. It depends upon the internet
connection.
Comments
The patient is a
child with rapidly progressive deterioration.
Surgical intervention is the best solution in
this case.
For detailed information about paragangliomas
please click
here!
Considering that the hearing is preserved and
the young age of the patient all efforts were
directed so as not to violate the bony
structures of the left ear and try with all
means to remove the tumor from the performed
approach, to avoid hearing disturbances.
The patient was discharged from ICU 04-June-2012
with rapidly recovering preoperative neurologic
deficits. Horner sign disappeared and swallowing
improved and no hiccup or strider and the
patient telling that hearing is normal and the
facial nerve function became normal.
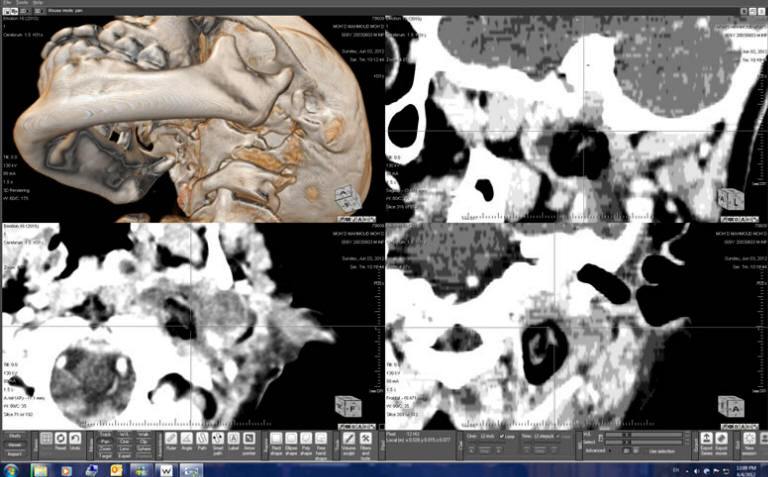
Postoperative CT-scan the second day after surgery with ORS Visual
reconstruction showing the tumor empty bed filled with air and
surgicele. Notice the intentionally left upper part of the tumor.
Notice: Not all operative activities
can be recorded due to lack of time.
Notice: Head injuries and very urgent surgeries are also
escaped from the plan .